

Magnetic resonance imaging radiomics predicts preoperative axillary lymph node metastasis to support surgical decisions and is associated with tumor microenvironment in invasive breast cancer: A machine learning, multicenter study
- PMID: 34233259
- PMCID: PMC8261009
- DOI: 10.1016/j.ebiom.2021.103460
Magnetic resonance imaging radiomics predicts preoperative axillary lymph node metastasis to support surgical decisions and is associated with tumor microenvironment in invasive breast cancer: A machine learning, multicenter study
Abstract
Background: in current clinical practice, the standard evaluation for axillary lymph node (ALN) status in breast cancer has a low efficiency and is based on an invasive procedure that causes operative-associated complications in many patients. Therefore, we aimed to use machine learning techniques to develop an efficient preoperative magnetic resonance imaging (MRI) radiomics evaluation approach of ALN status and explore the association between radiomics and the tumor microenvironment in patients with early-stage invasive breast cancer.
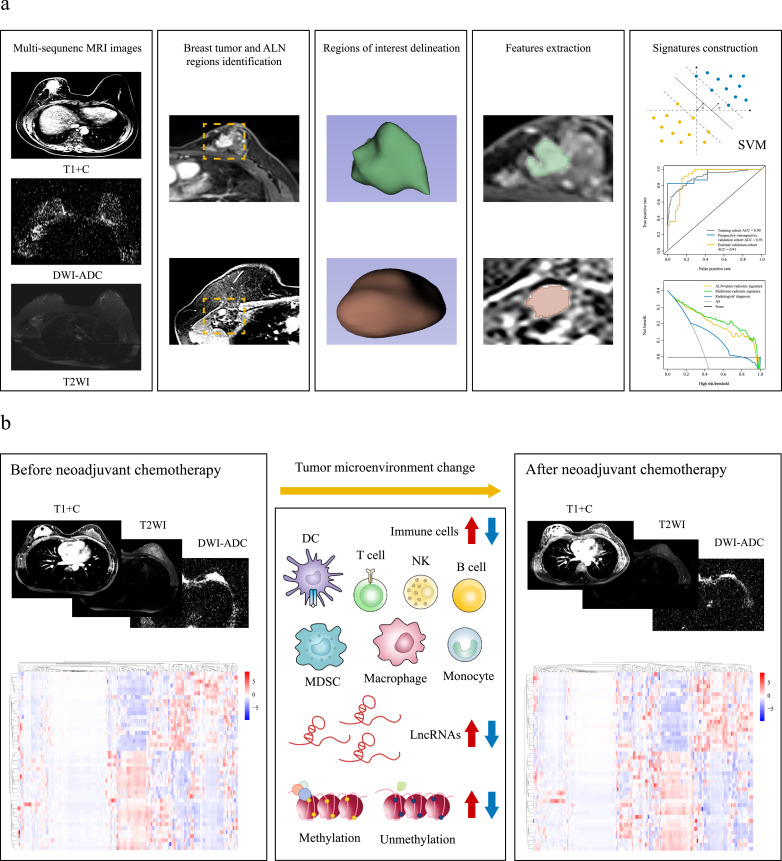
Methods: in this retrospective multicenter study, three independent cohorts of patients with breast cancer (n = 1,088) were used to develop and validate signatures predictive of ALN status. After applying the machine learning random forest algorithm to select the key preoperative MRI radiomic features, we used ALN and tumor radiomic features to develop the ALN-tumor radiomic signature for ALN status prediction by the support vector machine algorithm in 803 patients with breast cancer from Sun Yat-sen Memorial Hospital and Sun Yat-sen University Cancer Center (training cohort). By combining ALN and tumor radiomic features with corresponding clinicopathologic information, the multiomic signature was constructed in the training cohort. Next, the external validation cohort (n = 179) of patients from Shunde Hospital of Southern Medical University and Tungwah Hospital of Sun Yat-Sen University, and the prospective-retrospective validation cohort (n = 106) of patients treated with neoadjuvant chemotherapy in prospective phase 3 trials [NCT01503905], were included to evaluate the predictive value of the two signatures, and their predictive performance was assessed by the area under operating characteristic curve (AUC). This study was registered with ClinicalTrials.gov, number NCT04003558.
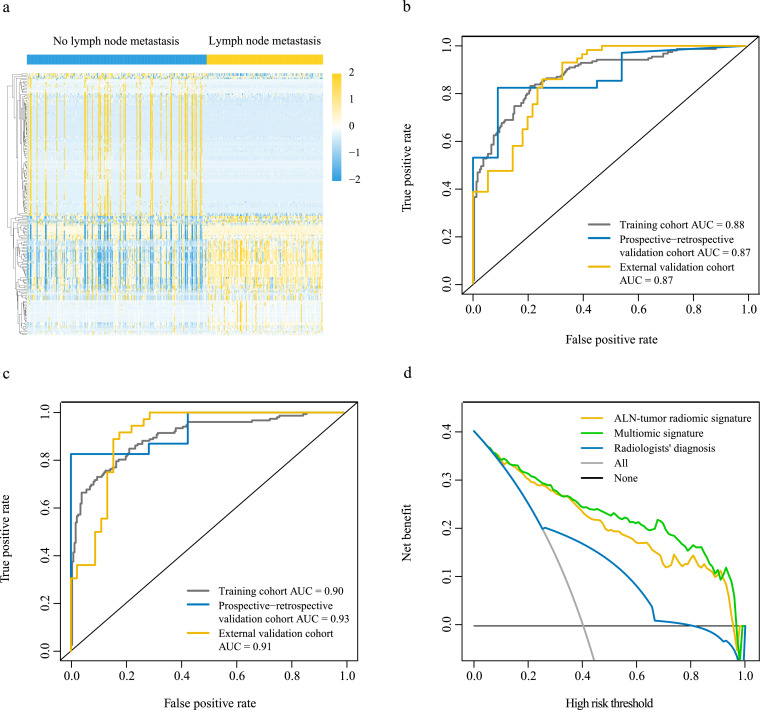
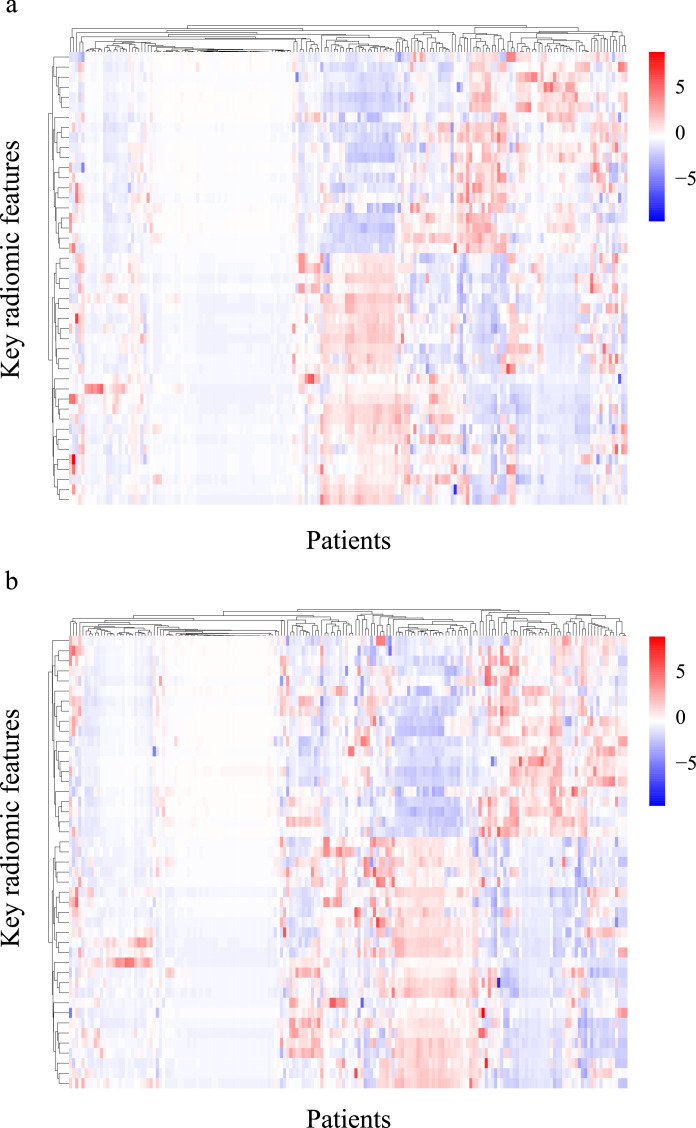
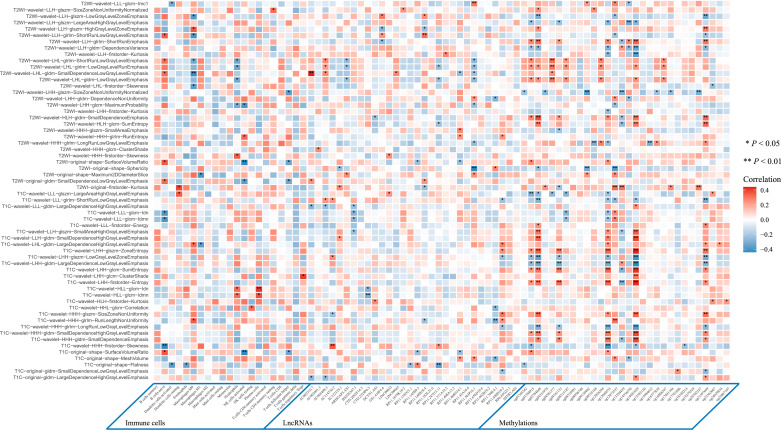
Findings: the ALN-tumor radiomic signature for ALN status prediction comprising ALN and tumor radiomic features showed a high prediction quality with AUC of 0·88 in the training cohort, 0·87 in the external validation cohort, and 0·87 in the prospective-retrospective validation cohort. The multiomic signature incorporating tumor and lymph node MRI radiomics, clinical and pathologic characteristics, and molecular subtypes achieved better performance for ALN status prediction with AUCs of 0·90, 0·91, and 0·93 in the training cohort, the external validation cohort, and the prospective-retrospective validation cohort, respectively. Among patients who underwent neoadjuvant chemotherapy in the prospective-retrospective validation cohort, there were significant differences in the key radiomic features before and after neoadjuvant chemotherapy, especially in the gray-level dependence matrix features. Furthermore, there was an association between MRI radiomics and tumor microenvironment features including immune cells, long non-coding RNAs, and types of methylated sites. Interpretation this study presented a multiomic signature that could be preoperatively and conveniently used for identifying patients with ALN metastasis in early-stage invasive breast cancer. The multiomic signature exhibited powerful predictive ability and showed the prospect of extended application to tailor surgical management. Besides, significant changes in key radiomic features after neoadjuvant chemotherapy may be explained by changes in the tumor microenvironment, and the association between MRI radiomic features and tumor microenvironment features may reveal the potential biological underpinning of MRI radiomics.
Funding: No funding.
Keywords: Axillary lymph node metastasis; Breast cancer; Machine learning; Radiomics; Tumor microenvironment.
Copyright © 2021 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest We declare no conflicts of interest.
Figures
References
-
- Galimberti V., Bernard F., Viale G. Axillary dissection versus no axillary dissection in patients with breast cancer and sentinel-node micrometastases (IBCSG 23-01): 10-year follow-up of a randomized, controlled phase 3 trial. Lancet Oncol. 2018;19(10):1385–1393. - PubMed
-
- Lyman G.H., Giuliano A.E., Somerfield M.R. American society of clinical oncology guideline recommendations for sentinel lymph node biopsy in early-stage breast cancer. J Clin Oncol. 2005;23(30):7703–7720. - PubMed
-
- Gary H., Mark R., Linda D., Cheryl L., Donald L., Armando E. Sentinel lymph node biopsy for patients with early-stage breast cancer: American society of clinical oncology clinical practice guideline update. J Clin Oncol. 2017;35(5):561–564. - PubMed
-
- Giammarile F., Alazraki N., Aarsvold J.N. The EANM and SNMMI practice guideline for lymphoscintigraphy and sentinel node localization in breast cancer. Eur J Nucl Med Mol Imaging. 2013;40(12):1932–1947. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
