

Analysis of left ventricular function, left ventricular outflow tract and aortic valve area using computed tomography: Influence of reconstruction parameters on measurement accuracy
- PMID: 34233477
- PMCID: PMC8523190
- DOI: 10.1259/bjr.20201306
Analysis of left ventricular function, left ventricular outflow tract and aortic valve area using computed tomography: Influence of reconstruction parameters on measurement accuracy
Abstract
Objectives: Computed tomography (CT) allows reproducible assessment of left ventricular (LV) function, left ventricular outflow tract area (LVOTarea) and aortic valve area (AVA). We evaluated the influence of image reconstruction parameters on these measurements.
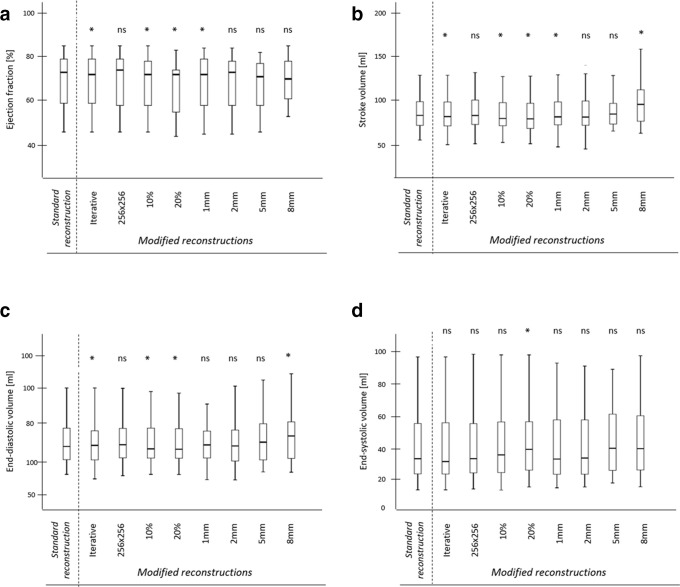
Methods: We analyzed 45 contrast-enhanced, retrospectively ECG-gated CT datasets acquired on a third-generation dual source system. A standard filtered-back-projection data set (20 cardiac phases (5% steps, 0-95%), 0.6-mm-slice thickness, 512 × 512 matrix) and eight reconstructions with modified slice thickness (1-8 mm), number of cardiac phases (5, 10), matrix size (256×256) and an iterative reconstruction (IR) algorithm were obtained. LV parameters (ejection fraction (EF), stroke volume (SV), end-diastolic (EDV), end-systolic volumes (ESV)), LVOTarea and AVA were assessed.
Results: Differences in LV parameters, LVOTarea and AVA, were only minimal between standard reconstructions and those with modified matrix size, IR algorithm and ≤2 mm slice thickness, while reconstructions with 8-mm slice thickness significantly overestimated SV (p < 0.001) and EDV (p = 0.016). AVA planimetry in reconstructions with ≥5 mm slice thickness was not feasible in 56% of patients. A decrease in the number of reconstructed phases (10 or 5) underestimated EF, SV, EDV, LVOTarea and AVA and overestimated ESV.
Conclusions: Modifications of reconstruction parameters (except a slice thickness ≤2 mm) have only a marginal effect on LV, LVOTarea and AVA assessment. However, a reduced number of reconstructions per cardiac cycle may significantly influence measurements.
Advances in knowledge: Substantial modifications in number of reconstructions per cardiac cycle significantly affect the assessment of LV function, LVOTarea and AVA also in modern CT scanners.
Conflict of interest statement
Figures






Similar articles
-
[Evaluation of two "fast" software tools for the measurement of left ventricular volumes in retrospectively ECG-gated multidetector CT of the heart: biplane area-length method and "shape tracking" method].Rofo. 2007 Jun;179(6):572-80. doi: 10.1055/s-2007-962864. Epub 2007 Mar 21. Rofo. 2007. PMID: 17377874 German.
-
Assessment of global left ventricular function with dual-source computed tomography in patients with valvular heart disease.Acta Radiol. 2012 Apr 1;53(3):270-7. doi: 10.1258/ar.2011.110247. Epub 2012 Feb 8. Acta Radiol. 2012. PMID: 22319133
-
Assessment of global left ventricular systolic function with multidetector CT and 2D echocardiography: a comparison between reconstructions of 1-mm and 2-mm slice thickness at multidetector CT.Diagn Interv Radiol. 2010 Sep;16(3):236-40. doi: 10.4261/1305-3825.DIR.2624-09.2. Epub 2010 Jul 15. Diagn Interv Radiol. 2010. PMID: 20635319
-
Quantitative 4-dimensional volumetric analysis of left ventricle in ischemic heart disease by 64-slice computed tomography: a comparative study with invasive left ventriculogram.Int J Cardiol. 2008 Sep 16;129(1):42-52. doi: 10.1016/j.ijcard.2007.06.060. Epub 2007 Aug 20. Int J Cardiol. 2008. PMID: 17707526
-
Comparison of global left ventricular function using 20 phases with 10-phase reconstructions in multidetector-row computed tomography.Int J Cardiovasc Imaging. 2012 Mar;28(3):603-11. doi: 10.1007/s10554-011-9828-z. Epub 2011 Feb 26. Int J Cardiovasc Imaging. 2012. PMID: 21359518
Cited by
-
Temporal image compression in cardiac computed tomography: impact of temporal super resolution and noise reduction for assessing left ventricular function.Radiol Phys Technol. 2025 Aug 16. doi: 10.1007/s12194-025-00950-x. Online ahead of print. Radiol Phys Technol. 2025. PMID: 40817156
-
Minimal dose CT for left ventricular ejection fraction and combination with chest-abdomen-pelvis CT.Eur J Radiol Open. 2024 Jun 25;13:100583. doi: 10.1016/j.ejro.2024.100583. eCollection 2024 Dec. Eur J Radiol Open. 2024. PMID: 39026598 Free PMC article.
-
Potential for Dose Reduction in CT-Derived Left Ventricular Ejection Fraction: A Simulation Study.Tomography. 2023 Nov 15;9(6):2089-2102. doi: 10.3390/tomography9060164. Tomography. 2023. PMID: 37987350 Free PMC article.
-
Diagnostic Challenges in the Management of Aortic Valve Stenosis and the Role of Imaging: A Narrative Review.J Clin Med. 2025 Feb 13;14(4):1231. doi: 10.3390/jcm14041231. J Clin Med. 2025. PMID: 40004761 Free PMC article. Review.
References
-
- Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. . Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of echocardiography and the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging 2015; 16: 233–71. doi: 10.1093/ehjci/jev014 - DOI - PubMed
-
- Petersen SE, Khanji MY, Plein S, Lancellotti P, Bucciarelli-Ducci C. European association of cardiovascular imaging expert consensus paper: a comprehensive review of cardiovascular magnetic resonance normal values of cardiac chamber size and aortic root in adults and recommendations for grading severity. Eur Heart J Cardiovasc Imaging 2019; 20: 1321–31. doi: 10.1093/ehjci/jez232 - DOI - PubMed
-
- Shiran A, Adawi S, Ganaeem M, Asmer E. Accuracy and reproducibility of left ventricular outflow tract diameter measurement using transthoracic when compared with transesophageal echocardiography in systole and diastole. Eur J Echocardiogr 2009; 10: 319–24. doi: 10.1093/ejechocard/jen254 - DOI - PubMed
-
- Blanke P, Weir-McCall JR, Achenbach S, Delgado V, Hausleiter J, Jilaihawi H, et al. . Computed tomography imaging in the context of transcatheter aortic valve implantation (TAVI) / transcatheter aortic valve replacement (TAVR): an expert consensus document of the Society of cardiovascular computed tomography. J Cardiovasc Comput Tomogr 2019; 13: 1–20. doi: 10.1016/j.jcct.2018.11.008 - DOI - PubMed
