

Soft tissue masses of the epitrochlear region
- PMID: 34233485
- PMCID: PMC9328048
- DOI: 10.1259/bjr.20210236
Soft tissue masses of the epitrochlear region
Abstract
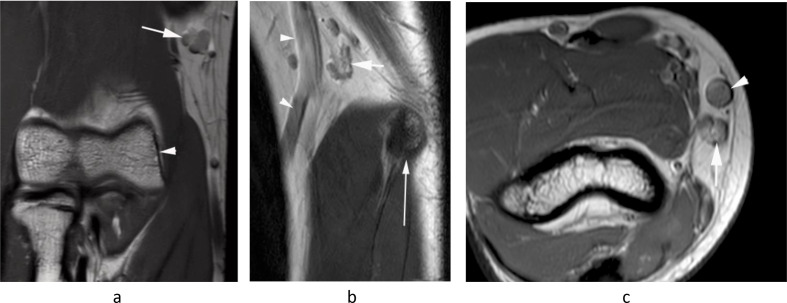
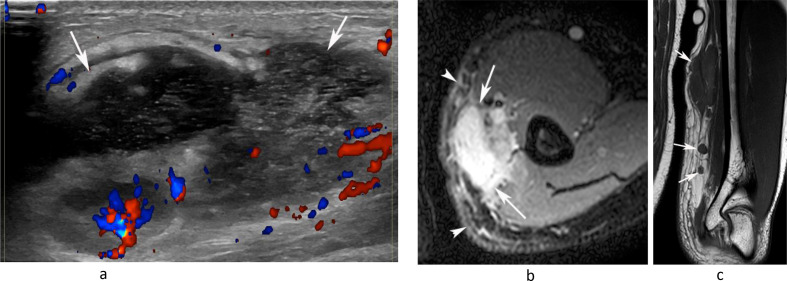
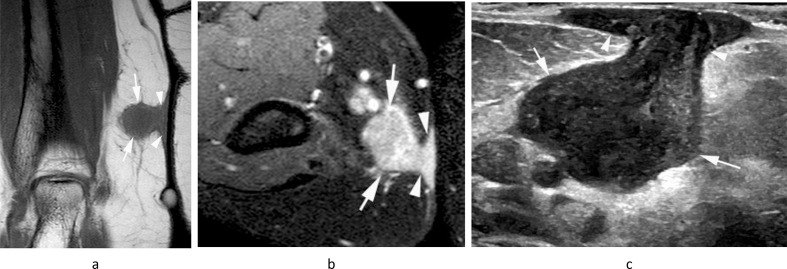
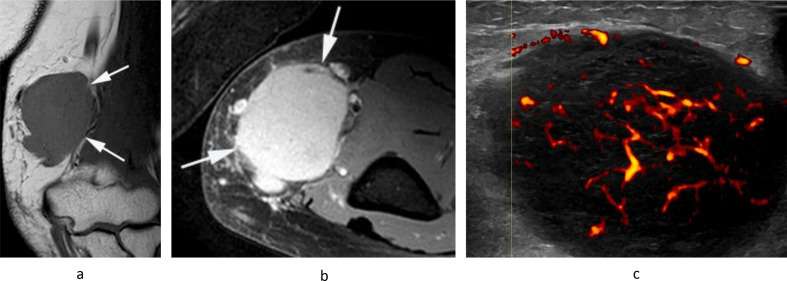
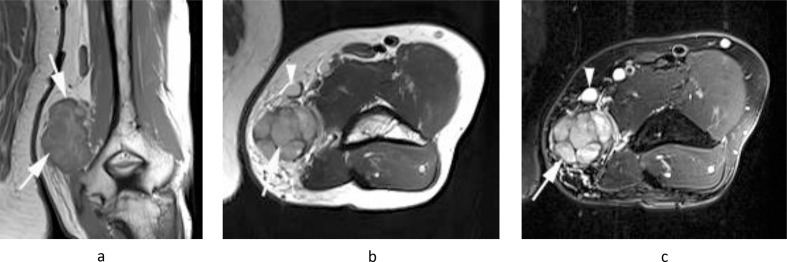
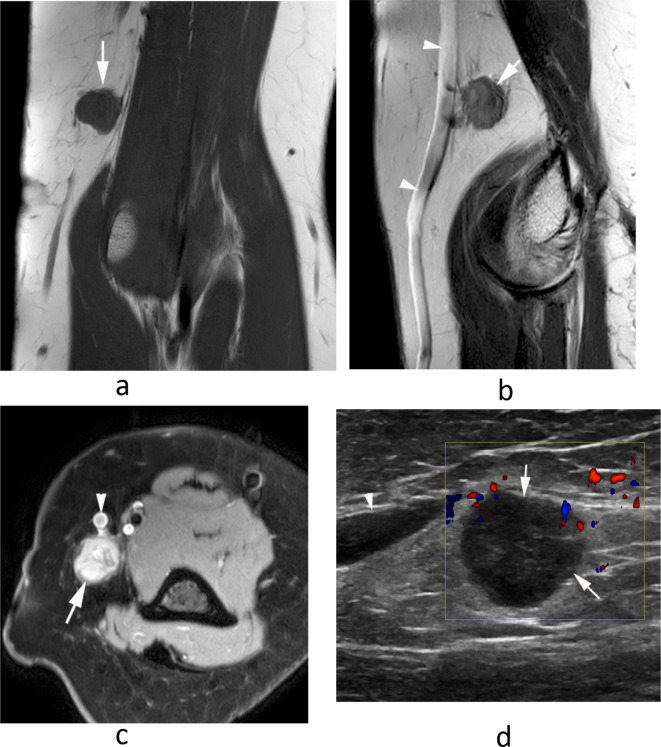
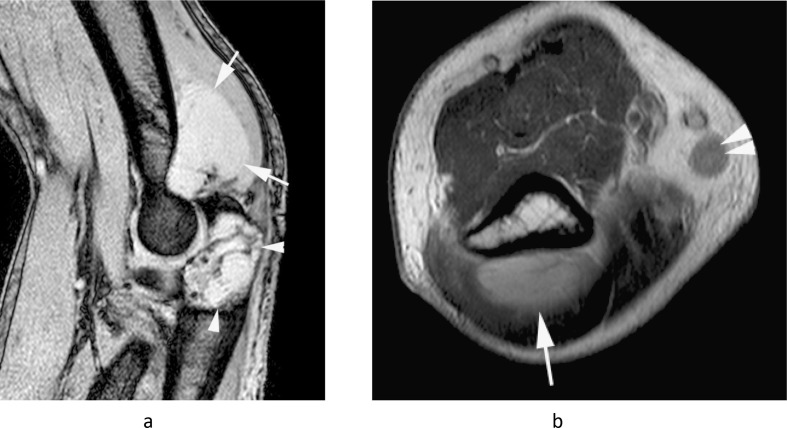
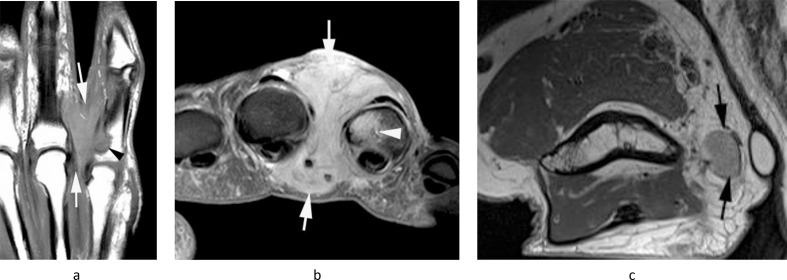
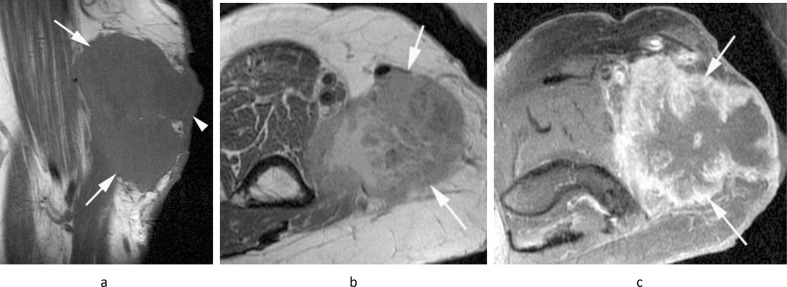
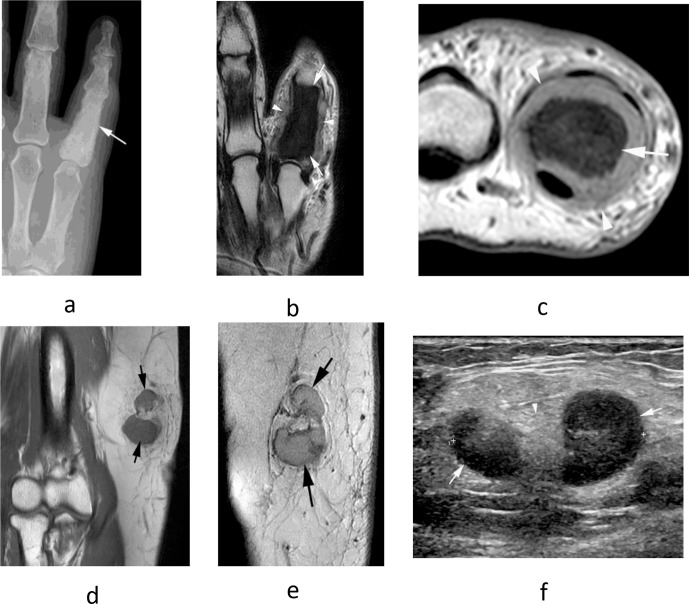
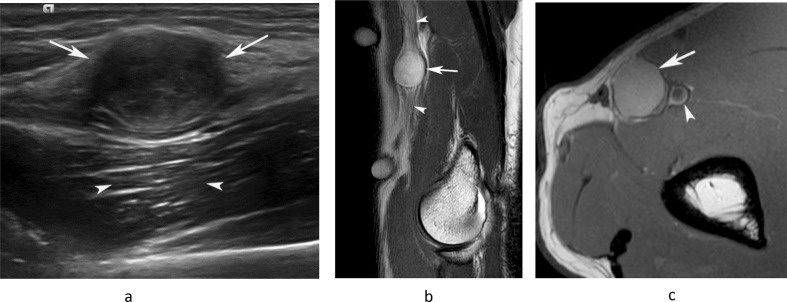
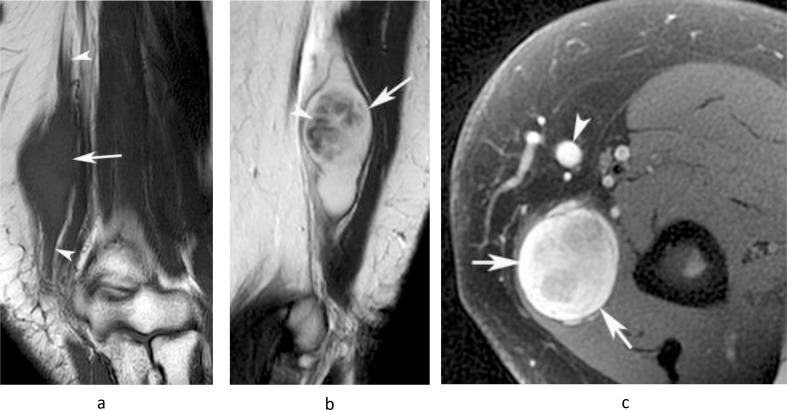
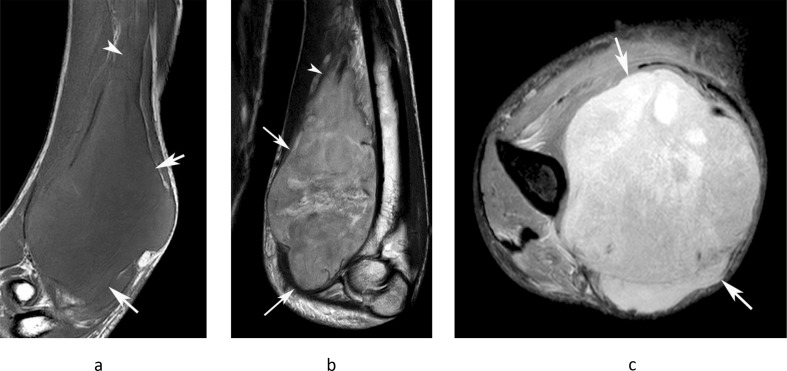
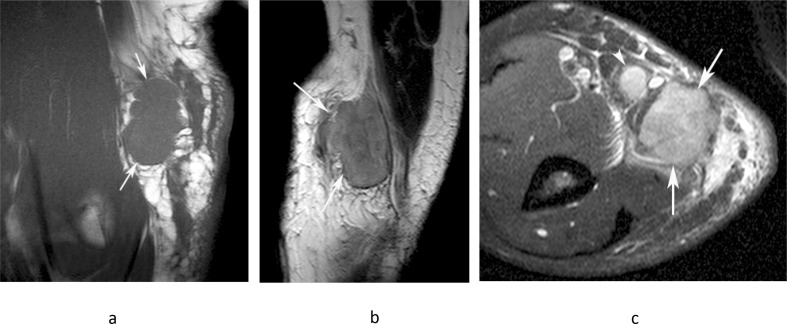
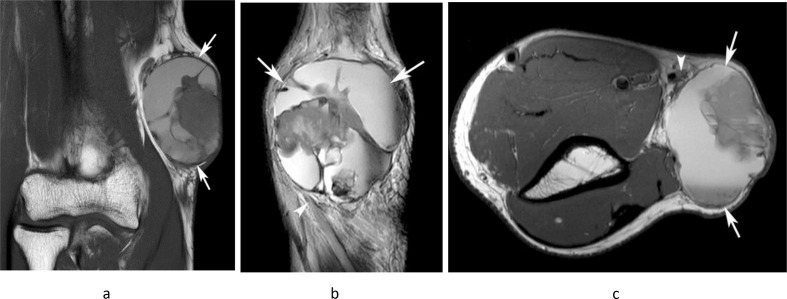
The epitrochlear lymph nodes (ELN) are rarely examined clinically and are difficult to identify radiologically in healthy patients. They are, therefore, generally under appreciated as a source of significant pathology. Despite this, enlargement of an ELN is almost always secondary to a pathological process, the differential for which is relatively narrow. The following pictorial review illustrates the spectrum of infectious, inflammatory and malignant conditions affecting the ELN, some of which are quite specific to this location. We also emphasise the importance of distinguishing enlarged ELNs from benign and malignant non-nodal soft tissue masses, which can have very similar clinical presentation and imaging appearances.
Figures
Similar articles
-
Pathologically Benign Lymph Nodes Can Mimic Malignancy on Imaging in Patients With Angiomatoid Fibrous Histiocytoma.Clin Orthop Relat Res. 2017 Sep;475(9):2274-2279. doi: 10.1007/s11999-017-5388-4. Epub 2017 May 23. Clin Orthop Relat Res. 2017. PMID: 28536856 Free PMC article.
-
A Pictorial Review of Sonography of Intramammary Lymph Nodes: When to Care and What to Do About It.Ultrasound Q. 2019 Mar;35(1):74-78. doi: 10.1097/RUQ.0000000000000395. Ultrasound Q. 2019. PMID: 30516732 Review.
-
Mid-arm sentinel lymph nodes showing surprising drainage from a malignant melanoma in the forearm.Clin Nucl Med. 1998 May;23(5):273-4. doi: 10.1097/00003072-199805000-00001. Clin Nucl Med. 1998. PMID: 9596149
-
Sonography of soft tissue masses of the neck.J Clin Ultrasound. 2002 Jul-Aug;30(6):356-73. doi: 10.1002/jcu.10073. J Clin Ultrasound. 2002. PMID: 12116098 Review.
-
Sentinel lymph node biopsy in pediatric soft tissue sarcoma patients: utility and concordance with imaging.J Pediatr Surg. 2013 Sep;48(9):1903-6. doi: 10.1016/j.jpedsurg.2013.04.013. J Pediatr Surg. 2013. PMID: 24074665
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
