

Buried bumper syndrome: a case report of an early PEG gastropexy-associated complication in a patient with gastric volvulus
- PMID: 34234941
- PMCID: PMC8257257
- DOI: 10.1093/jscr/rjab261
Buried bumper syndrome: a case report of an early PEG gastropexy-associated complication in a patient with gastric volvulus
Abstract
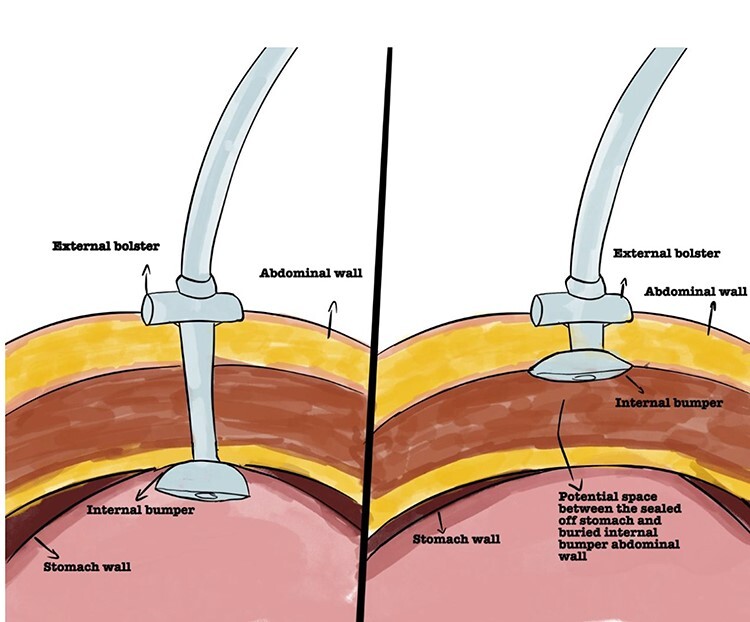
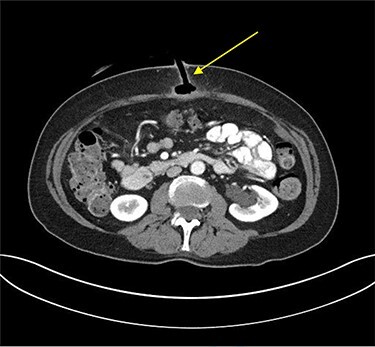
Buried bumper syndrome (BBS) is a rare complication associated with percutaneous endoscopic gastrostomy (PEG) tubes. It develops when the internal bumper migrates through the gastric wall, lodging anywhere along the gastrostomy tract leading to overgrowth of gastric mucosa thereby encasing the tube. BBS can lead to bleeding, perforation, peritonitis and intra-abdominal sepsis. Our case is a 71-year-old female presenting with tenderness, erythema and purulent discharge at the PEG tube site 2-weeks post-insertion. Computer tomography scan demonstrated the PEG had dislodged with the internal bumper in the subcutaneous tissue and the distal tip lying within the tract beyond the stomach wall. The PEG was removed by simple external traction. The patient clinically improved and discharged home on day three. Although BBS usually occurs late post-PEG insertion, it can also occur acutely. Preventative measures should be adopted at ward-level and emphasized with appropriate PEG tube care information provided to patients to avoid and recognize such complication.
Published by Oxford University Press and JSCR Publishing Ltd. © The Author(s) 2021.
Figures
References
-
- Gauderer MW, Ponsky JL, Izant RJ Jr. Gastrostomy without laparotomy: a percutaneous endoscopic technique. J Pediatr Surg 1980;15:872–5. - PubMed
-
- Kercher KW, Matthews BD, Ponsky JL, Goldstein SL, Yavorski RT, Sing RF, et al. Minimally invasive management of paraesophageal herniation in the high-risk surgical patient. Am J Surg 2001;182:510–4. - PubMed
-
- Nutrition BAfPaE . Percutaneous endoscopic gastrostomy management of buried bumper syndrome-decision tree. 2012.
-
- Lee TH, Lin JT. Clinical manifestations and management of buried bumper syndrome in patients with percutaneous endoscopic gastrostomy. Gastrointest Endosc 2008;68:580–4. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
