

Serologic Status and Toxic Effects of the SARS-CoV-2 BNT162b2 Vaccine in Patients Undergoing Treatment for Cancer
- PMID: 34236381
- PMCID: PMC8267843
- DOI: 10.1001/jamaoncol.2021.2675
Serologic Status and Toxic Effects of the SARS-CoV-2 BNT162b2 Vaccine in Patients Undergoing Treatment for Cancer
Abstract
Importance: The efficacy and safety profile of SARS-CoV-2 vaccines have been acquired from phase 3 studies; however, patients with cancer were not represented in these trials. Owing to the recommendation to prioritize high-risk populations for vaccination, further data are warranted.
Objective: To evaluate the use and safety of the BNT162b2 vaccine in patients undergoing treatment for cancer.
Design, setting, and participants: In January 2021, mass SARS-CoV-2 vaccination of high-risk populations, including patients with cancer, was initiated in Israel. This cohort study prospectively enrolled and followed up patients with cancer and healthy participants between January 15 and March 14, 2021. The study was conducted at the Division of Oncology of Rambam Health Care Campus, the major tertiary (referral) medical center of northern Israel. Participants included 232 patients with cancer who were receiving active treatment after the first and second doses of the BNT162b2 vaccine and 261 healthy, age-matched health care workers who served as controls.
Exposures: Serum samples were collected after each vaccine dose and in cases of seronegativity. Questionnaires regarding sociodemographic characteristics and adverse reactions were administered at serum collection. A regulatory agencies-approved assay was used to assess IgG at all time points. Patients' electronic medical records were reviewed for documentation of COVID-19 infection and results of blood cell counts, liver enzyme levels, and imaging studies.
Main outcomes and measures: Seroconversion rate after the first and second doses of the BNT162b2 vaccine and documented COVID-19 infection.
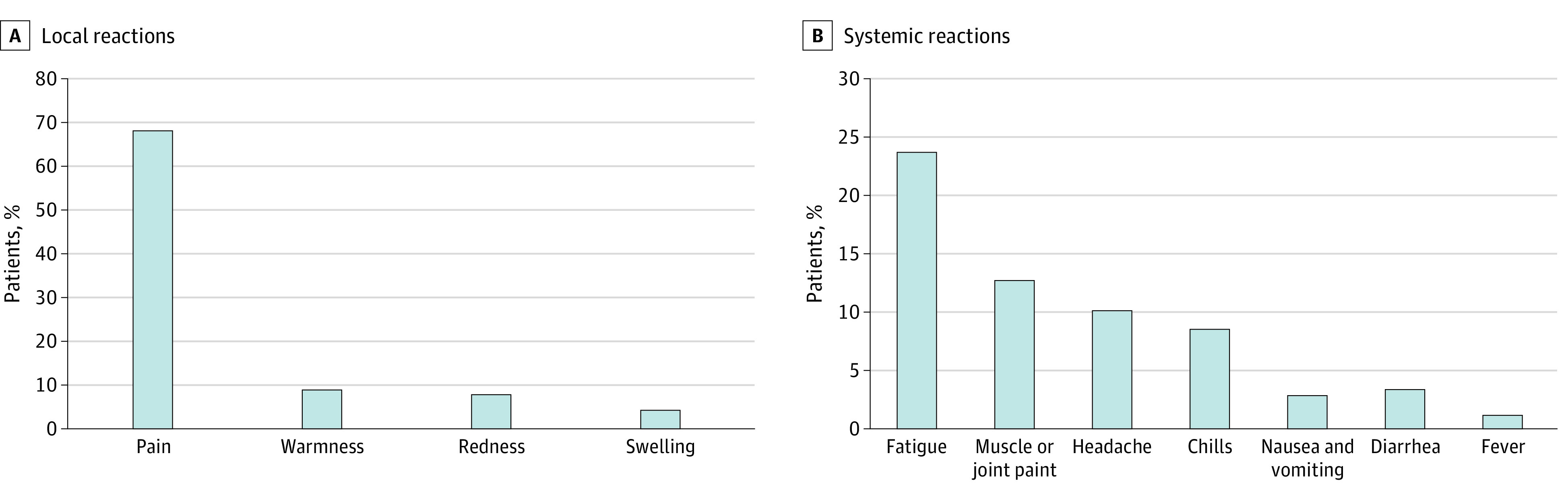
Results: Of the 232 patients undergoing treatment for cancer, 132 were men (57%); mean (SD) age was 66 (12.09) years. After the first dose of BNT162b2 vaccine, 29% (n = 25) patients were seropositive compared with 84% (n = 220) of the controls (P < .001). After the second dose, the seropositive rate reached 86% (n = 187) in the patients. Testing rate ratios per 1000 person-days after the first dose were 12.5 (95% CI, 3.4-45.7) for the patients and 48.5 (95% CI, 37.2-63.2) for the controls. Patients undergoing chemotherapy showed reduced immunogenicity (odds ratio, 0.41; 95% CI, 0.17-0.98). In seronegative patients, the rate of documented absolute leukopenia reached 39%. No COVID-19 cases were documented throughout the study period; however, 2 cases in the patient cohort were noted immediately after the first dose. Reported adverse events were similar to data in former trials comprising mostly healthy individuals.
Conclusions and relevance: In this cohort study, the SARS-CoV-2 BNT162b2 vaccine appeared to be safe and achieve satisfactory serologic status in patients with cancer. There was a pronounced lag in antibody production compared with the rate in noncancer controls; however, seroconversion occurred in most patients after the second dose. Future real-world data are warranted to determine the long-term efficacy of the vaccine with regard to type of anticancer treatment.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
