

Association of Combination of Conformation-Specific KIT Inhibitors With Clinical Benefit in Patients With Refractory Gastrointestinal Stromal Tumors: A Phase 1b/2a Nonrandomized Clinical Trial
- PMID: 34236401
- PMCID: PMC8267845
- DOI: 10.1001/jamaoncol.2021.2086
Association of Combination of Conformation-Specific KIT Inhibitors With Clinical Benefit in Patients With Refractory Gastrointestinal Stromal Tumors: A Phase 1b/2a Nonrandomized Clinical Trial
Abstract
Importance: Many cancer subtypes, including KIT-mutant gastrointestinal stromal tumors (GISTs), are driven by activating mutations in tyrosine kinases and may initially respond to kinase inhibitors but frequently relapse owing to outgrowth of heterogeneous subclones with resistance mutations. KIT inhibitors commonly used to treat GIST (eg, imatinib and sunitinib) are inactive-state (type II) inhibitors.
Objective: To assess whether combining a type II KIT inhibitor with a conformation-complementary, active-state (type I) KIT inhibitor is associated with broad mutation coverage and global disease control.
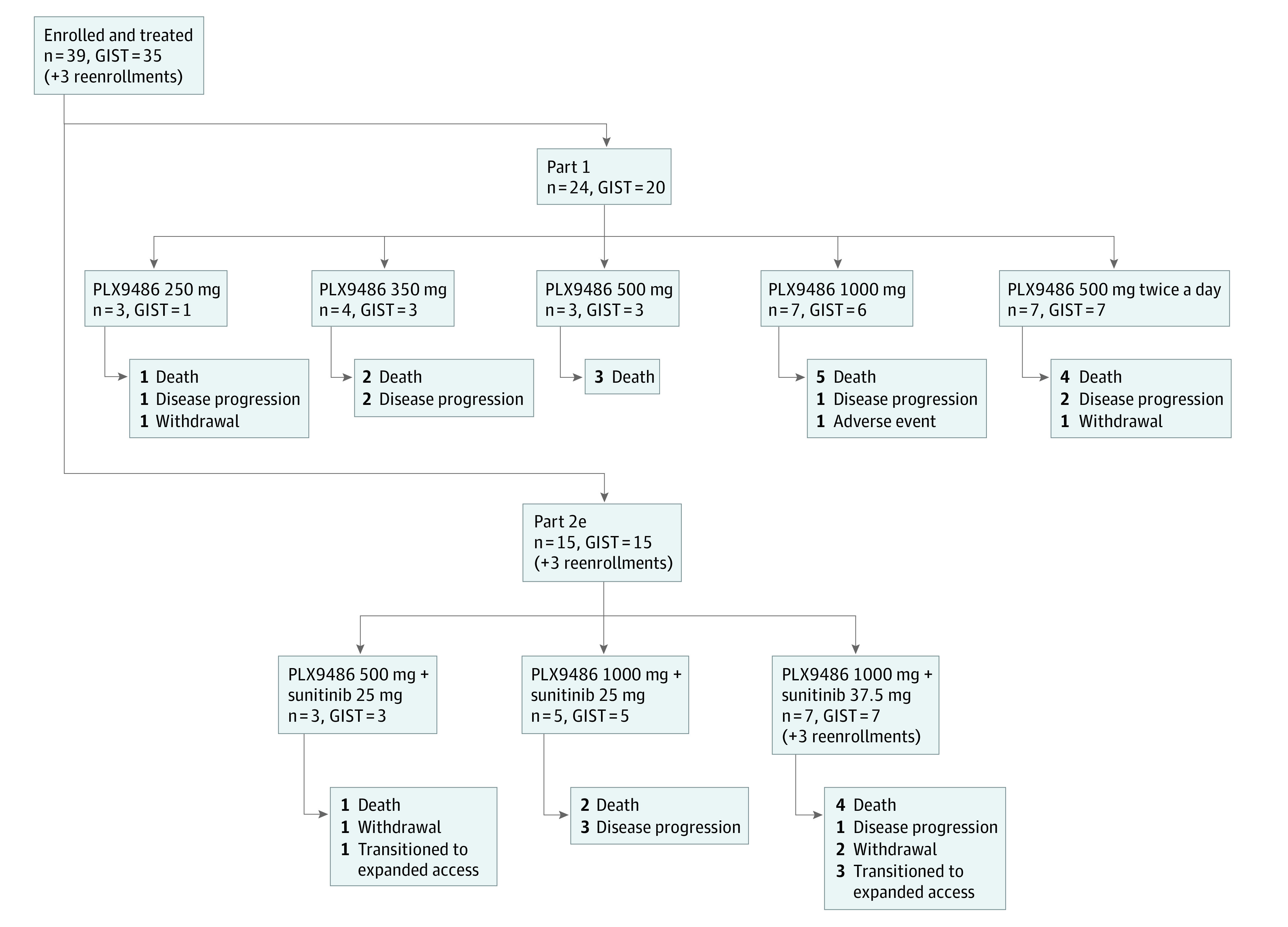
Design, setting, and participants: A highly selective type I inhibitor of KIT, PLX9486, was tested in a 2-part phase 1b/2a trial. Part 1 (dose escalation) evaluated PLX9486 monotherapy in patients with solid tumors. Part 2e (extension) evaluated PLX9486-sunitinib combination in patients with GIST. Patients were enrolled from March 2015 through February 2019; data analysis was performed from May 2020 through July 2020.
Interventions: Participants received 250, 350, 500, and 1000 mg of PLX9486 alone (part 1) or 500 and 1000 mg of PLX9486 together with 25 or 37.5 mg of sunitinib (part 2e) continuously in 28-day dosing cycles until disease progression, treatment discontinuation, or withdrawal.
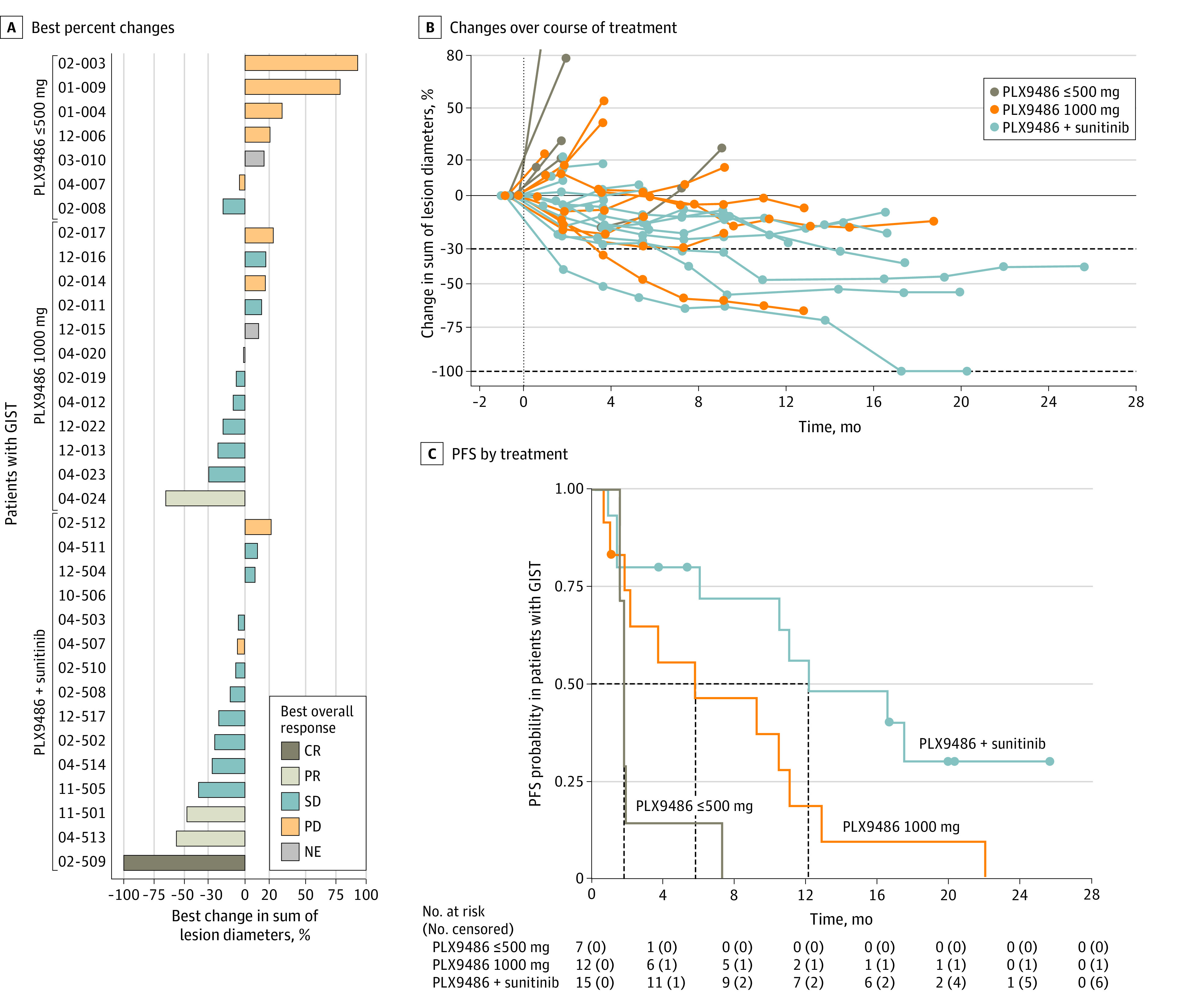
Main outcomes and measures: Pharmacokinetics, safety, and tumor responses were assessed. Clinical efficacy end points (progression-free survival and clinical benefit rate) were supplemented with longitudinal monitoring of KIT mutations in circulating tumor DNA.
Results: A total of 39 PLX9486-naive patients (median age, 57 years [range, 39-79 years]; 22 men [56.4%]; 35 [89.7%] with refractory GIST) were enrolled in the dose escalation and extension parts. The recommended phase 2 dose of PLX9486 was 1000 mg daily. At this dose, PLX9486 could be safely combined with 25 or 37.5 mg daily of sunitinib continuously. Patients with GIST who received PLX9486 at a dose of 500 mg or less, at the recommended phase 2 dose, and with sunitinib had median (95% CI) progression-free survivals of 1.74 (1.54-1.84), 5.75 (0.99-11.0), and 12.1 (1.34-NA) months and clinical benefit rates (95% CI) of 14% (0%-58%), 50% (21%-79%), and 80% (52%-96%), respectively.
Conclusions and relevance: In this phase 1b/2a nonrandomized clinical trial, type I and type II KIT inhibitors PLX9486 and sunitinib were safely coadministered at the recommended dose of both single agents in patients with refractory GIST. Results suggest that cotargeting 2 complementary conformational states of the same kinase was associated with clinical benefit with an acceptable safety profile.
Trial registration: ClinicalTrials.gov Identifier: NCT02401815.
Conflict of interest statement
Figures

References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
