

Adherence to Follow-up Testing Recommendations in US Veterans Screened for Lung Cancer, 2015-2019
- PMID: 34236409
- PMCID: PMC8267608
- DOI: 10.1001/jamanetworkopen.2021.16233
Adherence to Follow-up Testing Recommendations in US Veterans Screened for Lung Cancer, 2015-2019
Abstract
Importance: Lung cancer screening (LCS) can reduce lung cancer mortality with close follow-up and adherence to management recommendations. Little is known about factors associated with adherence to LCS in real-world practice, with data limited to case series from selected LCS programs.
Objective: To analyze adherence to follow-up based on standardized follow-up recommendations in a national cohort and to identify factors associated with delayed or absent follow-up.
Design, setting, and participants: This retrospective cohort study was conducted in Veterans Health Administration (VHA) facilities across the US. Veterans were screened for lung cancer between 2015 to 2019 with sufficient follow-up time to receive recommended evaluation. Patient- and facility-level logistic regression analyses were performed. Data were analyzed from November 26, 2019, to December 16, 2020.
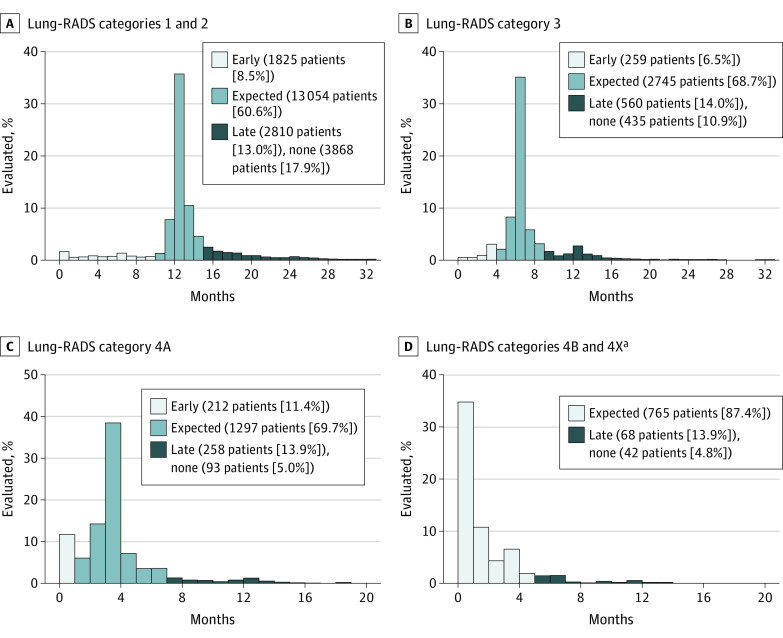
Main outcomes and measures: Receipt of the recommended next step after initial LCS according to Lung CT Screening Reporting & Data System (Lung-RADS) category, as captured in VHA or Medicare claims.
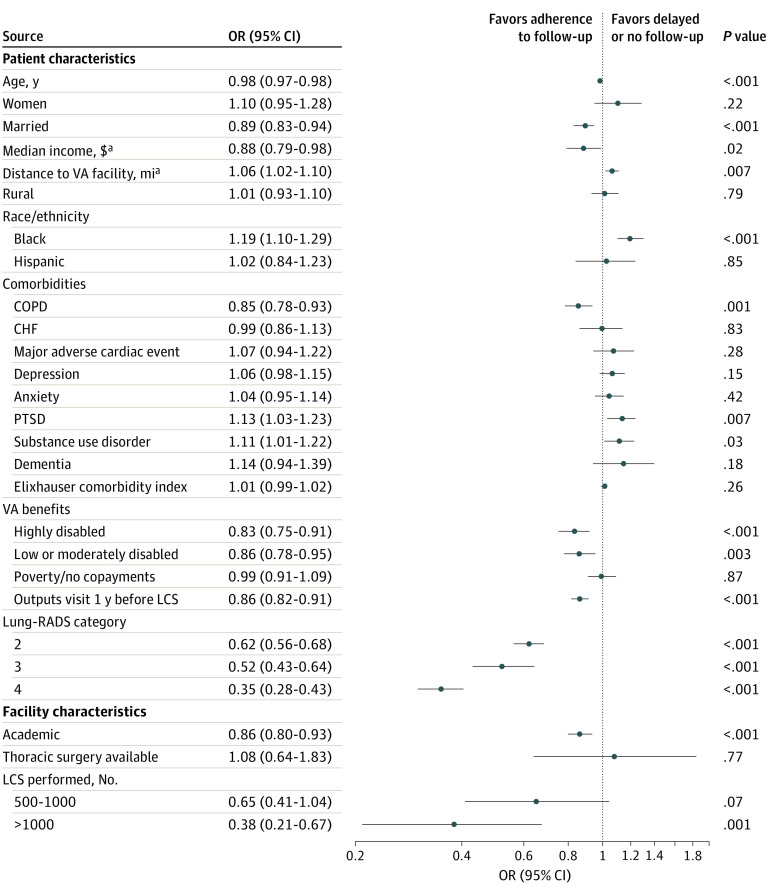
Results: Of 28 294 veterans (26 835 [94.8%] men; 21 969 individuals [77.6%] were White; mean [SD] age, 65.2 [5.5] years) who had an initial LCS examination, 17 863 veterans (63.1%) underwent recommended follow-up within the expected timeframe, whereas 3696 veterans (13.1%) underwent late evaluation, and 4439 veterans (15.7%) had no apparent evaluation. Facility-level differences were associated with 9.2% of the observed variation in rates of late or absent evaluation. In multivariable-adjusted models, Black veterans (odds ratio [OR], 1.19 [95% CI, 1.10-1.29]), veterans with posttraumatic stress disorder (OR, 1.13 [95% CI, 1.03-1.23]), veterans with substance use disorders (OR, 1.11 [95% CI, 1.01-1.22]), veterans with lower income (OR, 0.88 [95% CI, 0.79-0.98]), and those living at a greater distance from a VHA facility (OR, 1.06 [95% CI, 1.02-1.10]) were more likely to experience delayed or no follow-up; veterans with higher risk findings (Lung-RADS category 4 vs Lung-RADS category 1: OR, 0.35 [95% CI, 0.28-0.43]) and those screened in high LCS volume facilities (OR, 0.38 [95% CI, 0.21-0.67]) or academic facilities (OR, 0.86 [95% CI, 0.80-0.92]) were less likely to experience delayed or no follow-up. In sensitivity analyses, varying how stringently adherence was defined, expected evaluation ranged from 14 486 veterans (49.7%) under stringent definitions to 20 578 veterans (78.8%) under liberal definitions.
Conclusions and relevance: In this cohort study that captured follow-up care from the integrated VHA health care system and Medicare, less than two-thirds of patients received timely recommended follow-up after initial LCS, with higher risk of delayed or absent follow-up among marginalized populations, such as Black individuals, individuals with mental health disorders, and individuals with low income, that have long experienced disparities in lung cancer outcomes. Future work should focus on identifying facilities that promote high adherence and disseminating successful strategies to promote equity in LCS among marginalized populations.
Conflict of interest statement
Figures
Comment in
-
Beyond the AJR: Disparities in Lung Cancer Screening Adherence Persist in the Veterans Health Administration.AJR Am J Roentgenol. 2022 May;218(5):926. doi: 10.2214/AJR.21.26852. Epub 2021 Sep 29. AJR Am J Roentgenol. 2022. PMID: 35234498 No abstract available.
