

Human AGR2 Deficiency Causes Mucus Barrier Dysfunction and Infantile Inflammatory Bowel Disease
- PMID: 34237462
- PMCID: PMC8551217
- DOI: 10.1016/j.jcmgh.2021.07.001
Human AGR2 Deficiency Causes Mucus Barrier Dysfunction and Infantile Inflammatory Bowel Disease
Erratum in
-
Corrections.Cell Mol Gastroenterol Hepatol. 2024;17(4):670. doi: 10.1016/j.jcmgh.2024.02.005. Epub 2024 Feb 21. Cell Mol Gastroenterol Hepatol. 2024. PMID: 38383221 Free PMC article. No abstract available.
Abstract
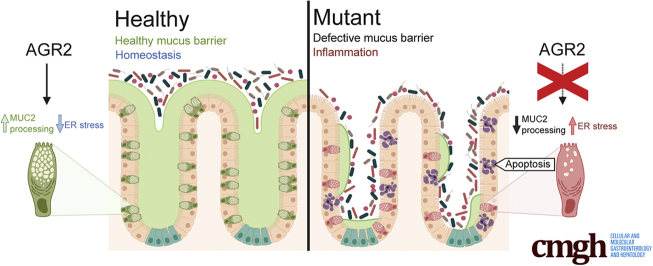
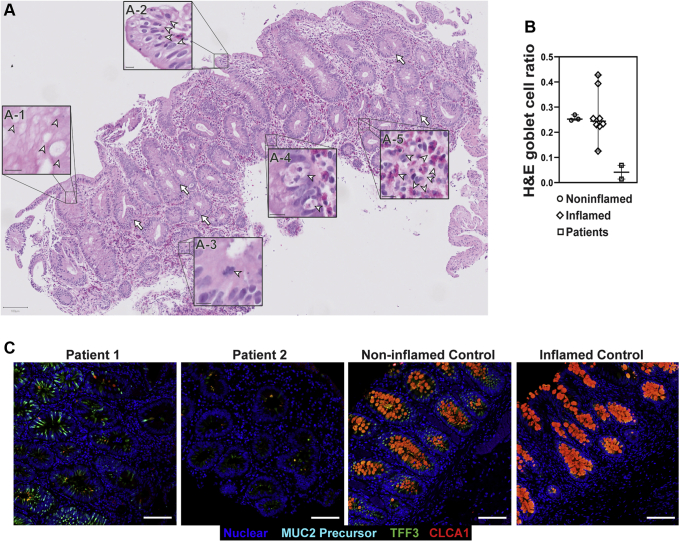
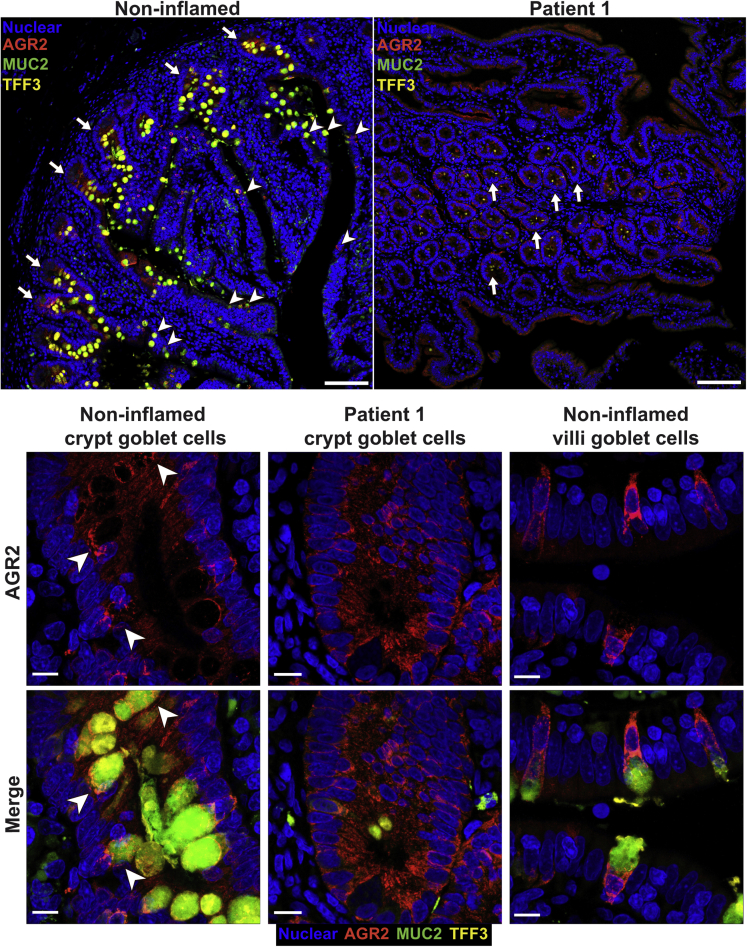
Background & aims: The gastrointestinal epithelium plays a crucial role in maintaining homeostasis with the gut microbiome. Mucins are essential for intestinal barrier function and serve as a scaffold for antimicrobial factors. Mucin 2 (MUC2) is the major intestinal gel-forming mucin produced predominantly by goblet cells. Goblet cells express anterior gradient 2 (AGR2), a protein disulfide isomerase that is crucial for proper processing of gel-forming mucins. Here, we investigated 2 siblings who presented with severe infantile-onset inflammatory bowel disease.
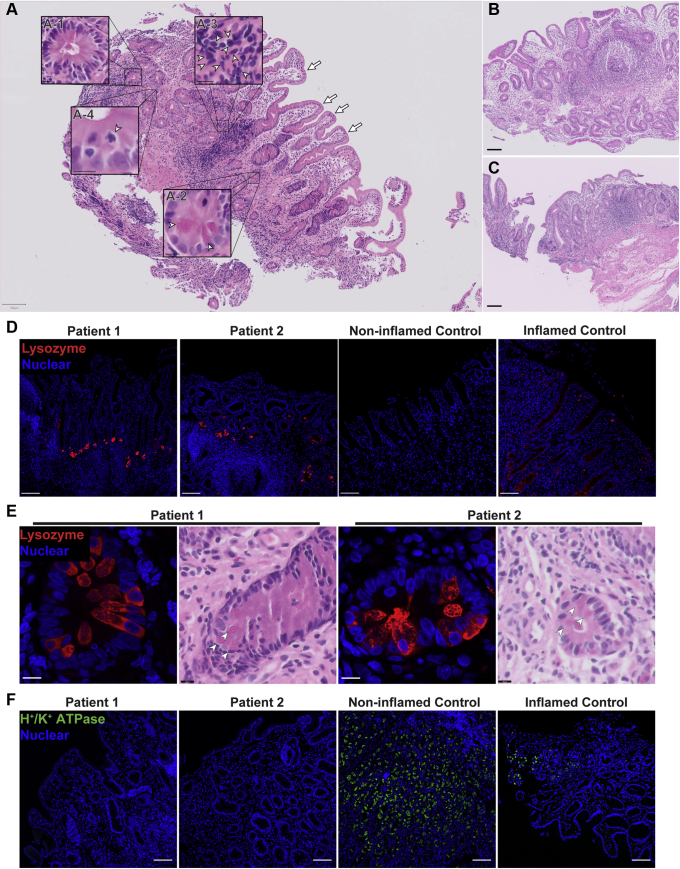
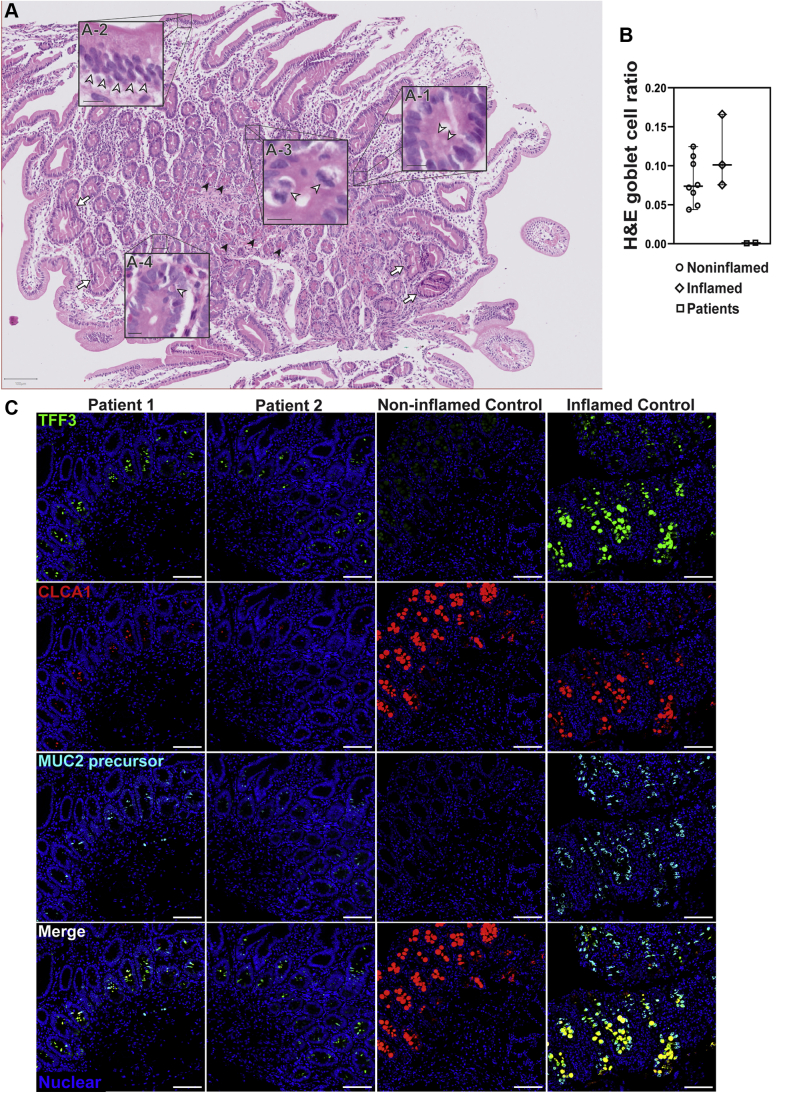
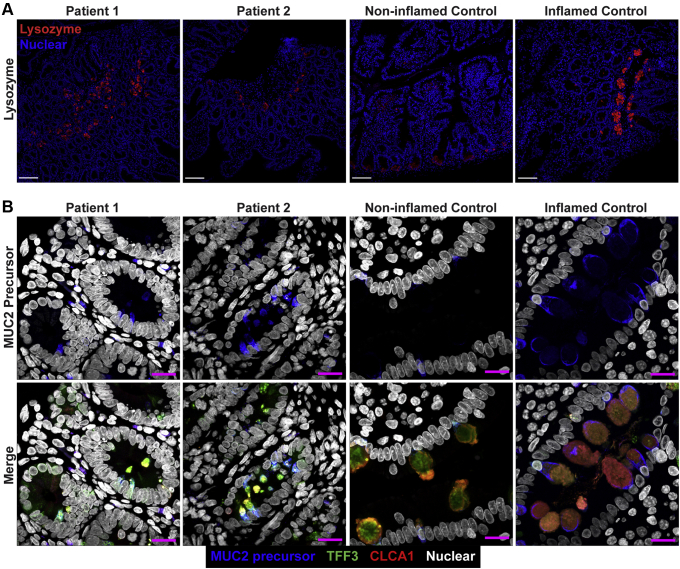
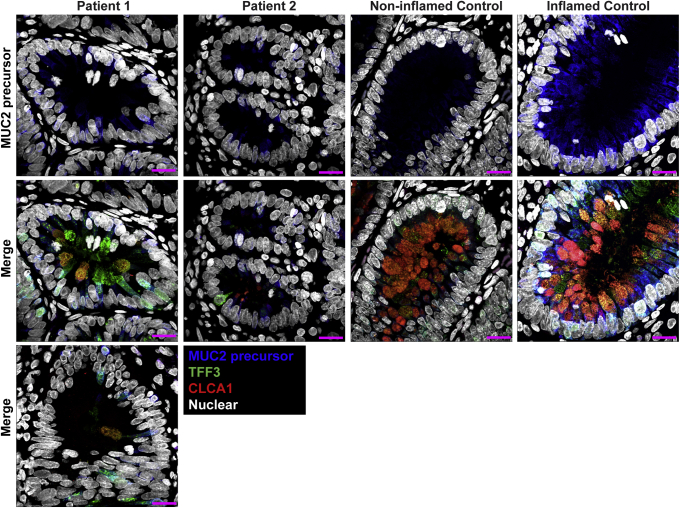
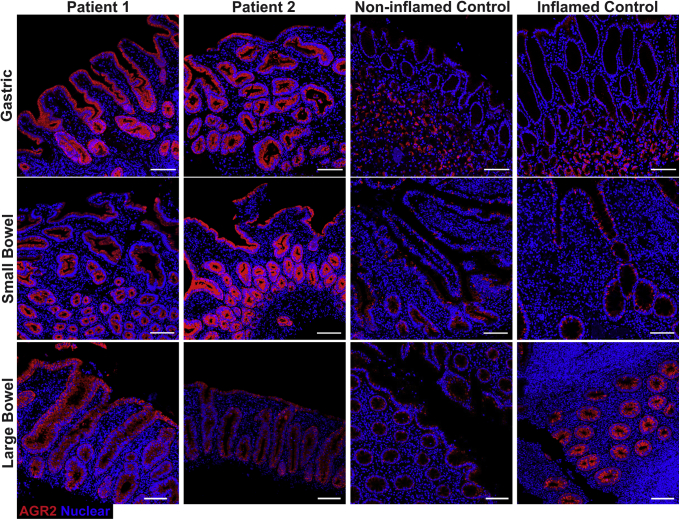
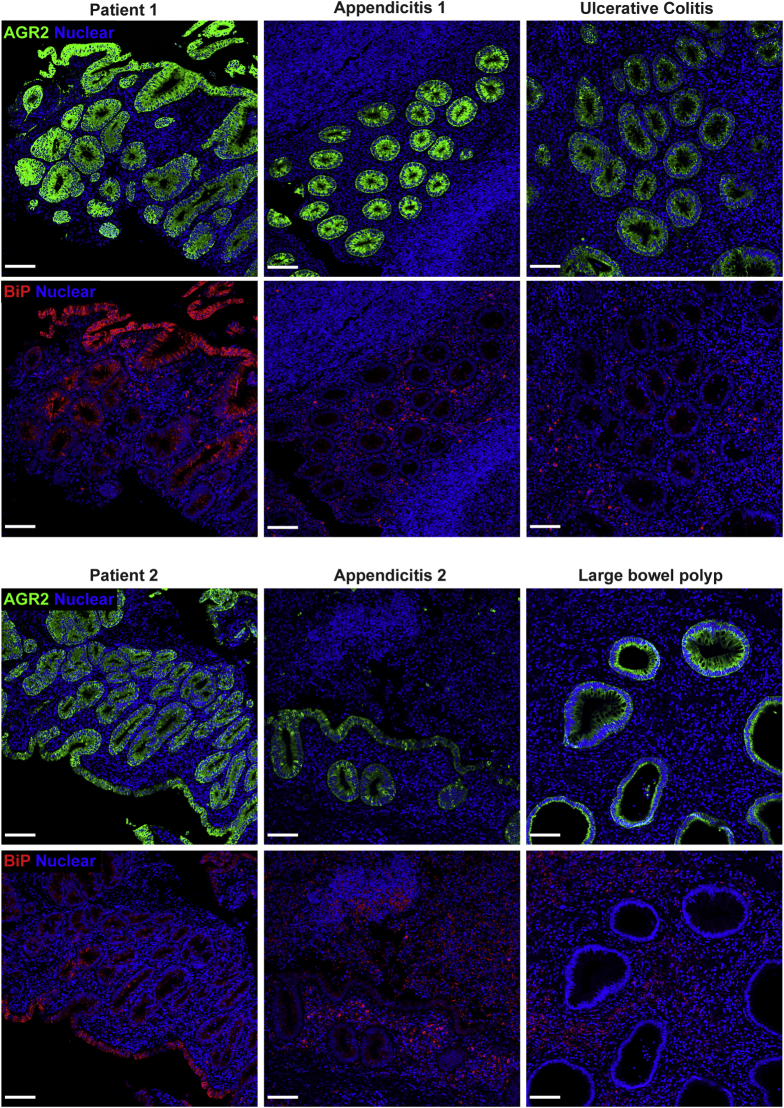
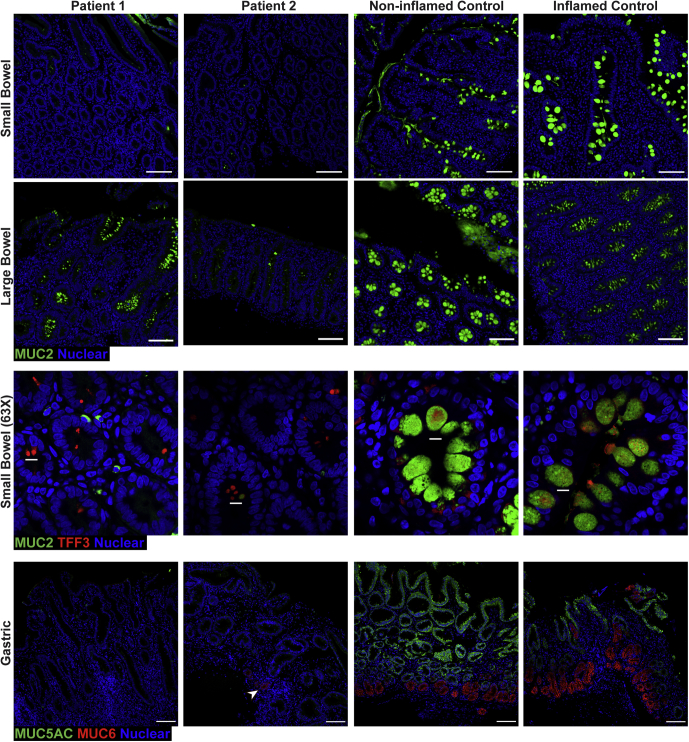
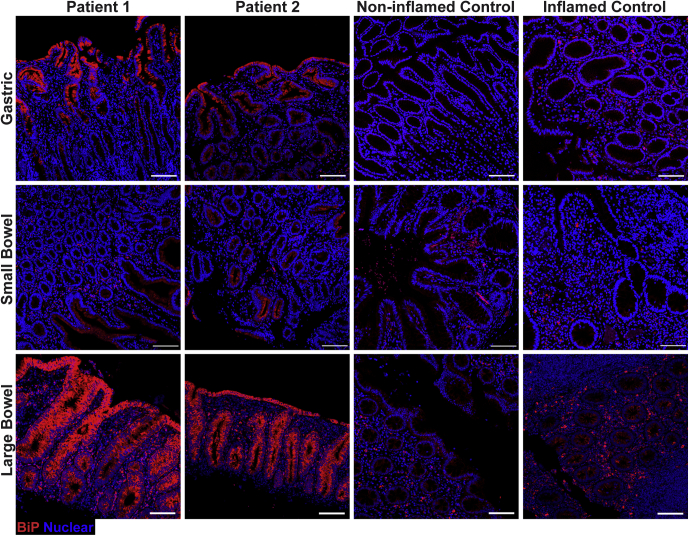
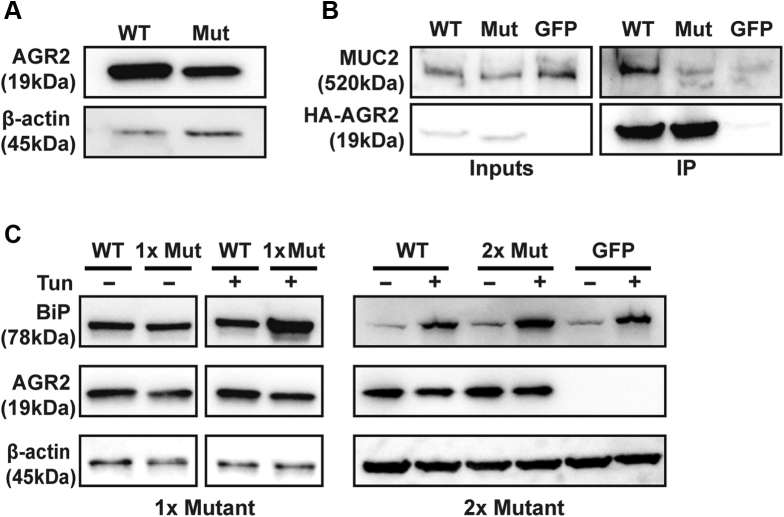
Methods: We performed whole-genome sequencing to identify candidate variants. We quantified goblet cell numbers using H&E histology and investigated the expression of gel-forming mucins, stress markers, and goblet cell markers using immunohistochemistry. AGR2-MUC2 binding was evaluated using co-immunoprecipitation. Endoplasmic reticulum (ER) stress regulatory function of mutant AGR2 was examined by expression studies in Human Embryonic Kidney 293T (HEK293T) using tunicamycin to induce ER stress.
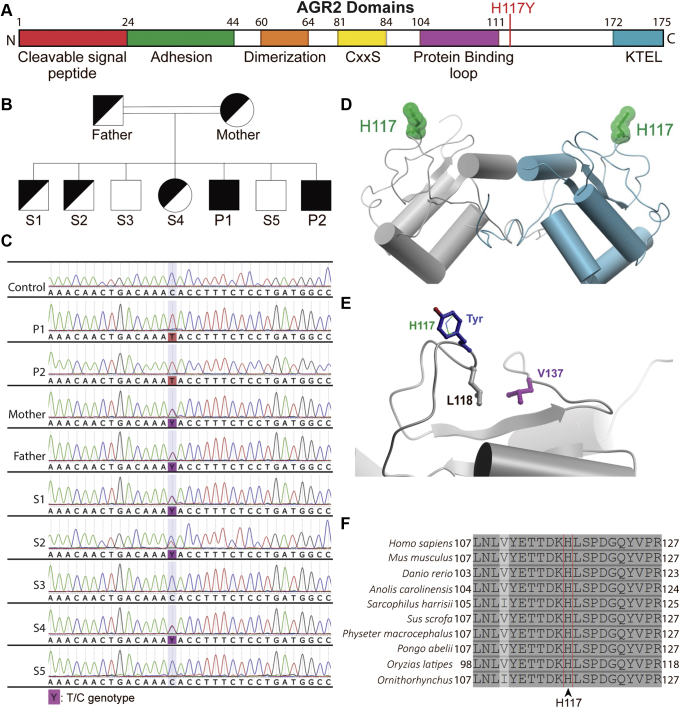
Results: Both affected siblings were homozygous for a missense variant in AGR2. Patient biopsy specimens showed reduced goblet cells; depletion of MUC2, MUC5AC, and MUC6; up-regulation of AGR2; and increased ER stress. The mutant AGR2 showed reduced capacity to bind MUC2 and alleviate tunicamycin-induced ER stress.
Conclusions: Phenotype-genotype segregation, functional experiments, and the striking similarity of the human phenotype to AGR2-/- mouse models suggest that the AGR2 missense variant is pathogenic. The Mendelian deficiency of AGR2, termed "Enteropathy caused by AGR2 deficiency, Goblet cell Loss, and ER Stress" (EAGLES), results in a mucus barrier defect, the inability to mitigate ER stress, and causes infantile-onset inflammatory bowel disease.
Keywords: AGR2; ER Stress; Goblet Cells; Intestinal Metaplasia; MUC2.
Copyright © 2021 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Crowley E., Warner N., Pan J., Khalouei S., Elkadri A., Fiedler K., Foong J., Turinsky A.L., Bronte-Tinkew D., Zhang S., Hu J., Tian D., Li D., Horowitz J., Siddiqui I., Upton J., Roifman C.M., Church P.C., Wall D.A., Ramani A.K., Kotlarz D., Klein C., Uhlig H., Snapper S.B., Gonzaga-Jauregui C., Paterson A.D., McGovern D.P.B., Brudno M., Walters T.D., Griffiths A.M., Muise A.M. Prevalence and clinical features of inflammatory bowel diseases associated with monogenic variants, identified by whole-exome sequencing in 1000 children at a single center. Gastroenterology. 2020;158:2208–2220. - PMC - PubMed
-
- Hooper L.V., MacPherson A.J. Immune adaptations that maintain homeostasis with the intestinal microbiota. Nat Rev Immunol. 2010;10:159–169. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Miscellaneous
