

Efficacy and Tolerability of Combination Treatments for Major Depression: Antidepressants plus Second-Generation Antipsychotics vs. Esketamine vs. Lithium
- PMID: 34238049
- PMCID: PMC8358538
- DOI: 10.1177/02698811211013579
Efficacy and Tolerability of Combination Treatments for Major Depression: Antidepressants plus Second-Generation Antipsychotics vs. Esketamine vs. Lithium
Abstract
Background: Successful treatment of major depressive disorder (MDD) can be challenging, and failures ("treatment-resistant depression" [TRD]) are frequent. Steps to address TRD include increasing antidepressant dose, combining antidepressants, adding adjunctive agents, or using nonpharmacological treatments. Their relative efficacy and tolerability remain inadequately tested. In particular, the value and safety of increasingly employed second-generation antipsychotics (SGAs) and new esketamine, compared to lithium as antidepressant adjuncts remain unclear.
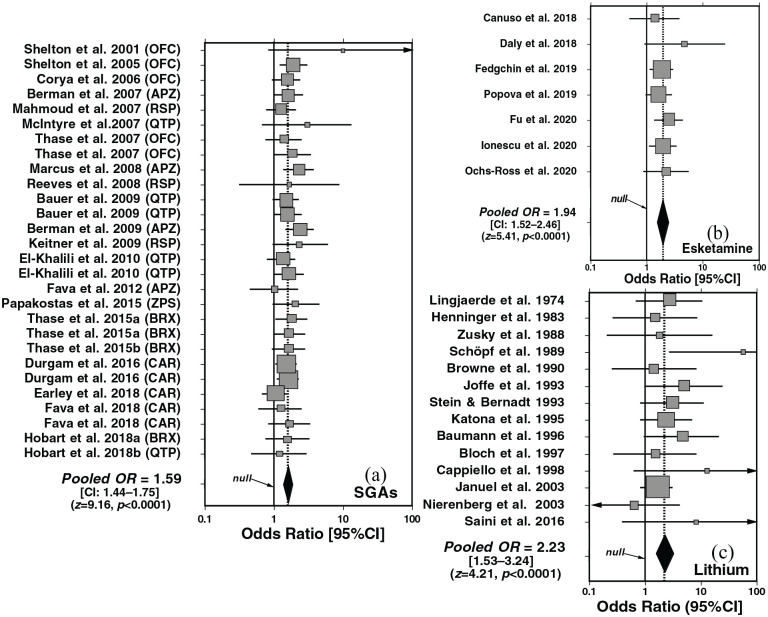
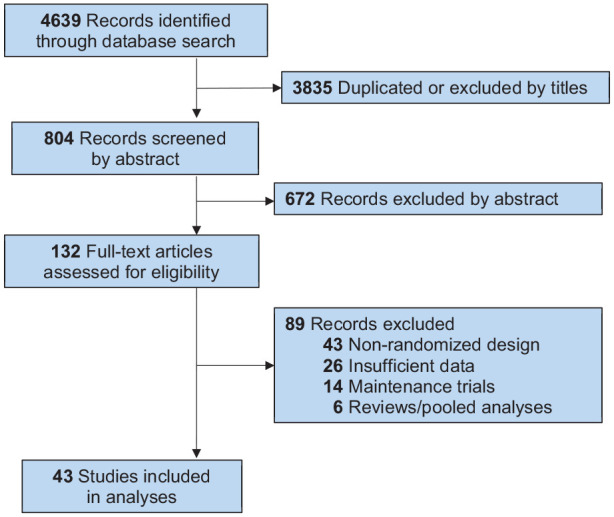
Methods: We reviewed randomized, placebo-controlled trials and used random-effects meta-analysis to compare odds ratio (OR) versus placebo, as well as numbers-needed-to-treat (NNT) and to-harm (NNH), for adding SGAs, esketamine, or lithium to antidepressants for major depressive episodes.
Results: Analyses involved 49 drug-placebo pairs. By NNT, SGAs were more effective than placebo (NNT = 11 [CI: 9-15]); esketamine (7 [5-10]) and lithium (5 [4-10]) were even more effective. Individually, aripiprazole, olanzapine+fluoxetine, risperidone, and ziprasidone all were more effective (all NNT < 10) than quetiapine (NNT = 13), brexpiprazole (16), or cariprazine (16), with overlapping NNT CIs. Risk of adverse effects, as NNH for most-frequently reported effects, among SGAs versus placebo was 5 [4-6] overall, and highest with quetiapine (NNH = 3), lowest with brexpiprazole (19), 5 (4-6) for esketamine, and 9 (5-106) with lithium. The risk/benefit ratio (NNH/NNT) was 1.80 (1.25-10.60) for lithium and much less favorable for esketamine (0.71 [0.60-0.80]) or SGAs (0.45 [0.17-0.77]).
Conclusions: Several modern antipsychotics and esketamine appeared to be useful adjuncts to antidepressants for acute major depressive episodes, but lithium was somewhat more effective and better tolerated.
Limitations: Most trials of adding lithium involved older, mainly tricyclic, antidepressants, and the dosing of adjunctive treatments were not optimized.
Keywords: Antidepressants; antipsychotics; combination; depression; efficacy; esketamine; lithium.
Conflict of interest statement
Figures
Comment in
-
A letter to the editor, associated with the article entitled "Efficacy and tolerability of combination treatments for major depression: Antidepressants plus second-generation antipsychotics vs esketamine vs lithium" by Vázquez et al. (Journal of Psychopharmacology, 2021, Vol. 35(8) 890-900).J Psychopharmacol. 2022 May;36(5):653-654. doi: 10.1177/02698811221092504. Epub 2022 Apr 27. J Psychopharmacol. 2022. PMID: 35475361 No abstract available.
Similar articles
-
Efficacy and tolerability of treatments for bipolar depression.J Affect Disord. 2015 Sep 1;183:258-62. doi: 10.1016/j.jad.2015.05.016. Epub 2015 May 19. J Affect Disord. 2015. PMID: 26042634
-
Efficacy and Safety of Intranasal Esketamine Adjunctive to Oral Antidepressant Therapy in Treatment-Resistant Depression: A Randomized Clinical Trial.JAMA Psychiatry. 2018 Feb 1;75(2):139-148. doi: 10.1001/jamapsychiatry.2017.3739. JAMA Psychiatry. 2018. PMID: 29282469 Free PMC article. Clinical Trial.
-
Balancing benefits and harms of treatments for acute bipolar depression.J Affect Disord. 2014 Dec;169 Suppl 1:S24-33. doi: 10.1016/S0165-0327(14)70006-0. J Affect Disord. 2014. PMID: 25533911 Review.
-
Treatment of bipolar depression: making sensible decisions.CNS Spectr. 2014 Dec;19 Suppl 1:4-11; quiz 1-3, 12. doi: 10.1017/S109285291400056X. Epub 2014 Nov 19. CNS Spectr. 2014. PMID: 25407667 Review.
-
Efficacy of Esketamine Nasal Spray Plus Oral Antidepressant Treatment for Relapse Prevention in Patients With Treatment-Resistant Depression: A Randomized Clinical Trial.JAMA Psychiatry. 2019 Sep 1;76(9):893-903. doi: 10.1001/jamapsychiatry.2019.1189. JAMA Psychiatry. 2019. PMID: 31166571 Free PMC article. Clinical Trial.
Cited by
-
Understanding the habenula: A major node in circuits regulating emotion and motivation.Pharmacol Res. 2023 Apr;190:106734. doi: 10.1016/j.phrs.2023.106734. Epub 2023 Mar 16. Pharmacol Res. 2023. PMID: 36933754 Free PMC article. Review.
-
The Potential Use of Ebselen in Treatment-Resistant Depression.Pharmaceuticals (Basel). 2022 Apr 16;15(4):485. doi: 10.3390/ph15040485. Pharmaceuticals (Basel). 2022. PMID: 35455482 Free PMC article. Review.
-
Esketamine Nasal Spray: Rapid Relief for TRD and Suicide Prevention-Mechanisms and Pharmacodynamics.Neuropsychiatr Dis Treat. 2024 Nov 1;20:2059-2071. doi: 10.2147/NDT.S486118. eCollection 2024. Neuropsychiatr Dis Treat. 2024. PMID: 39502383 Free PMC article. Review.
-
The treatment of depression - searching for new ideas.Front Pharmacol. 2022 Oct 7;13:988648. doi: 10.3389/fphar.2022.988648. eCollection 2022. Front Pharmacol. 2022. PMID: 36278184 Free PMC article. Review.
-
Treatment-resistant depression: molecular mechanisms and management.Mol Biomed. 2024 Oct 17;5(1):43. doi: 10.1186/s43556-024-00205-y. Mol Biomed. 2024. PMID: 39414710 Free PMC article. Review.
References
-
- Baldessarini RJ. (2013) Chemotherapy in Psychiatry: Pharmacologic Basis of Treatments for Major Mental Illness, 3rd edn. New York, NY: Springer-Verlag.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
