

Effect of arterial oxygen partial pressure inflection point on Venoarterial extracorporeal membrane oxygenation for emergency cardiac support
- PMID: 34238331
- PMCID: PMC8268543
- DOI: 10.1186/s13049-021-00902-5
Effect of arterial oxygen partial pressure inflection point on Venoarterial extracorporeal membrane oxygenation for emergency cardiac support
Abstract
Background: Temporary circulatory support is a bridge between acute circulatory failure and definitive treatment or recovery. Currently, venoarterial extracorporeal membrane oxygenation (VA-ECMO) is considered to be one of the effective circulatory support methods, although cardiac function monitoring during the treatment still needs further investigation. Inflection point of arterial oxygen partial pressure (IPPaO2) may occur at an early stage in part of patients with a good prognosis after VA-ECMO treatment, and the relationship between time of IPPaO2 (tIPPaO2) and recovery of cardiac function or prognosis remains unclear.
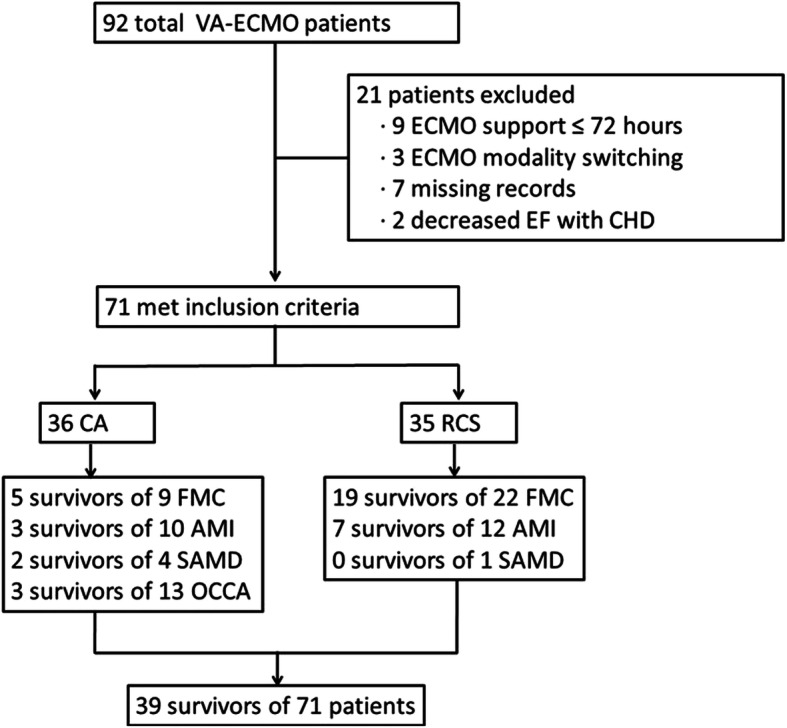
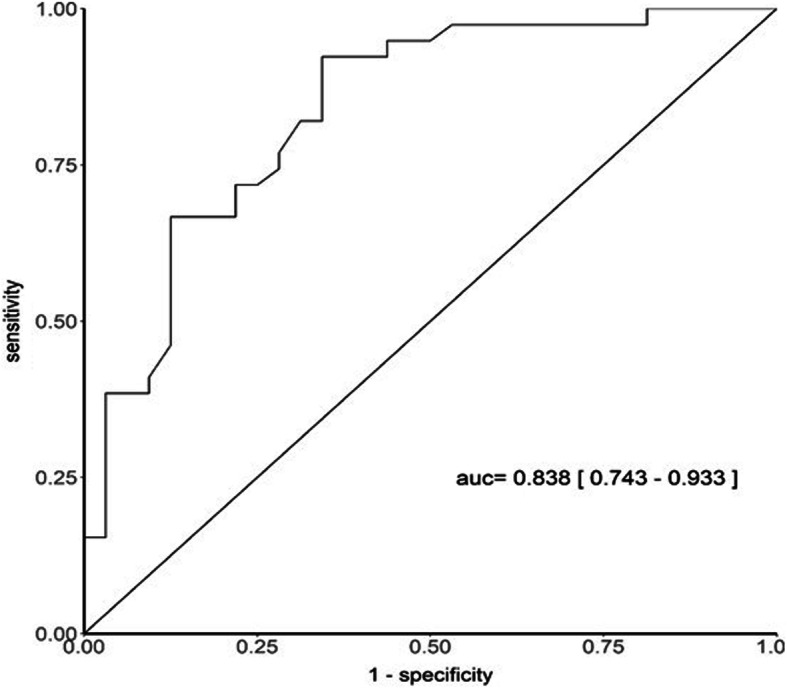
Methods: To investigate this relationship, we retrospectively analyzed the clinical data of 71 patients with different conditions after treatment with VA-ECMO in the emergency center of Jiangsu Province Hospital between May 2015 and July 2020. Spearman's correlation analysis was used for the correlation between tIPPaO2 and quantitative data, and ROC curve for the predictive effect of tIPPaO2 on the 28-day mortality.
Results: Thirty-five patients were admitted because of refractory cardiogenic shock (26 of 35 survived) and the remaining 36 patients due to cardiac arrest (13 of 36 survived). The overall survival rate was 54.9% (39 of 71 survived). Acute physiology and chronic health evaluation II, ECMO time, tIPPaO2, continuous renal replacement therapy time, mechanical ventilation time, and bleeding complications in the survival group were lower than those in the non-survival group, with length of stay, intensive care unit stay, and platelet levels were being higher. The tIPPaO2 was negatively correlated with ejection fraction, and the shorter tIPPaO2 resulted in a higher 28-day survival probability, higher predictive value for acute myocardial infarction and fulminant myocarditis.
Conclusions: Therefore, tIPPaO2 could be a reliable qualitative indicator of cardiac function in patients treated with VA-ECMO, which can reveal appropriate timing for adjusting VA-ECMO flow or weaning.
Trial registration: ChiCTR1900026105 .
Keywords: Cardiac arrest; Cardiac function; Refractory cardiogenic shock; VA-ECMO; tIPPaO2.
Conflict of interest statement
All authors declare no conflicts of interest.
Figures

References
-
- Ponikowski P, Voors AA, Anker SD, ESC Scientific Document Group et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37:2129–2200. doi: 10.1093/eurheartj/ehw128. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
