

Ablation Versus Drug Therapy for Atrial Fibrillation in Racial and Ethnic Minorities
- PMID: 34238436
- PMCID: PMC8354144
- DOI: 10.1016/j.jacc.2021.04.092
Ablation Versus Drug Therapy for Atrial Fibrillation in Racial and Ethnic Minorities
Abstract
Background: Rhythm control strategies for atrial fibrillation (AF), including catheter ablation, are substantially underused in racial/ethnic minorities in North America.
Objectives: This study sought to describe outcomes in the CABANA trial as a function of race/ethnicity.
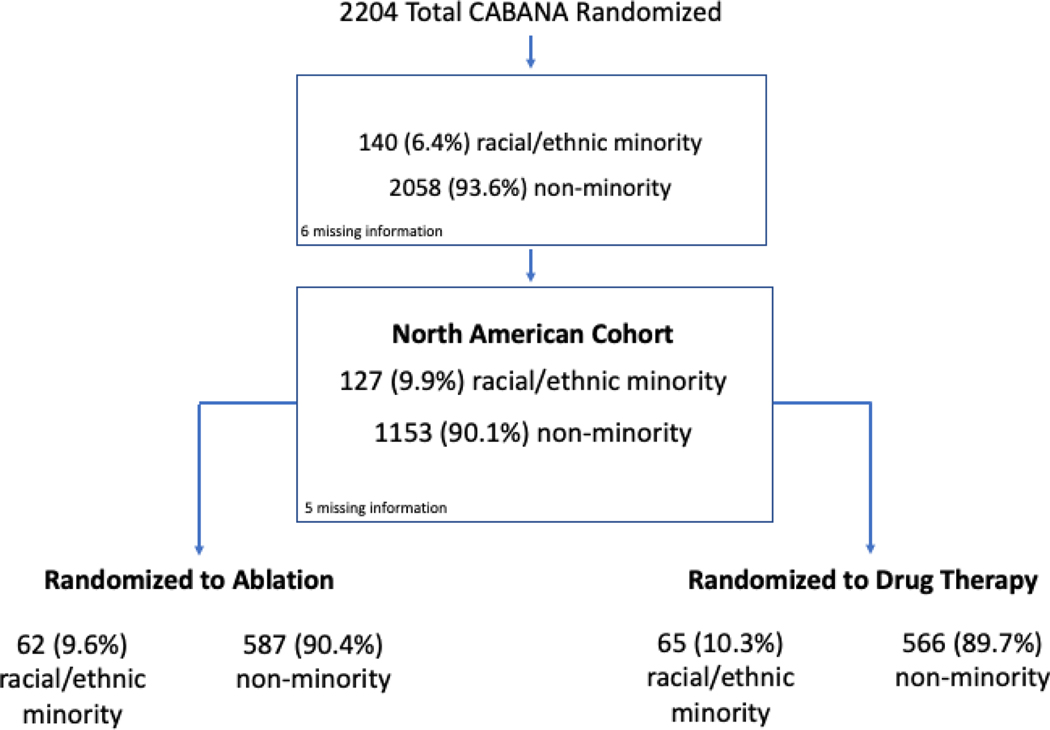
Methods: CABANA randomized 2,204 symptomatic participants with AF to ablation or drug therapy including rate and/or rhythm control drugs. Only participants in North America were included in the present analysis, and participants were subgrouped as racial/ethnic minority or nonminority with the use of National Institutes of Health definitions. The primary endpoint was a composite of death, disabling stroke, serious bleeding, or cardiac arrest.
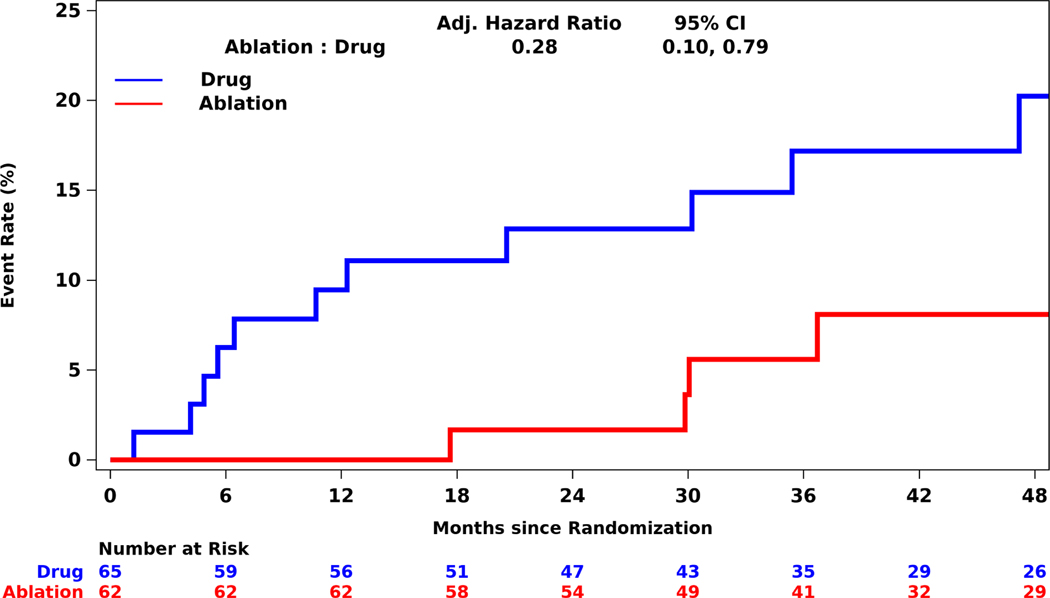
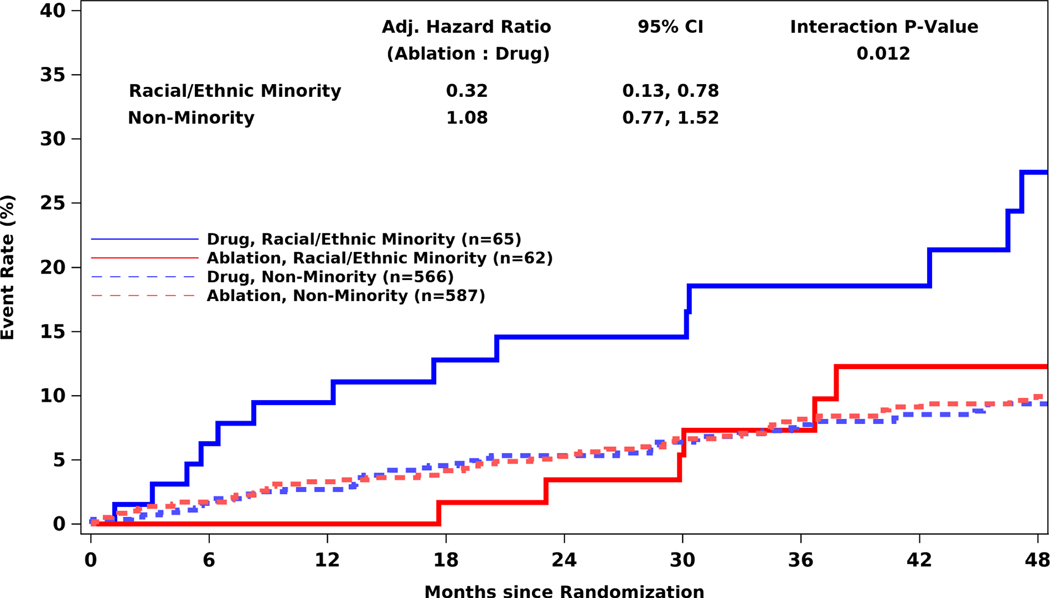
Results: Of 1,280 participants enrolled in CABANA in North America, 127 (9.9%) were racial and ethnic minorities. Compared with nonminorities, racial and ethnic minorities were younger with median age 65.6 versus 68.5 years, respectively, and had more symptomatic heart failure (37.0% vs 22.0%), hypertension (92.1% vs 76.8%, respectively), and ejection fraction <40% (20.8% vs 7.1%). Racial/ethnic minorities treated with ablation had a 68% relative reduction in the primary endpoint (adjusted hazard ratio [aHR]: 0.32; 95% confidence interval [CI]: 0.13-0.78) and a 72% relative reduction in all-cause mortality (aHR: 0.28; 95% CI: 0.10-0.79). Primary event rates in racial/ethnic minority and nonminority participants were similar in the ablation arm (4-year Kaplan-Meier event rates 12.3% vs 9.9%); however, racial and ethnic minorities randomized to drug therapy had a much higher event rate than nonminority participants (27.4% vs. 9.4%).
Conclusion: Among racial or ethnic minorities enrolled in the North American CABANA cohort, catheter ablation significantly improved major clinical outcomes compared with drug therapy. These benefits, which were not seen in nonminority participants, appear to be due to worse outcomes with drug therapy. (Catheter Ablation vs Anti-arrhythmic Drug Therapy for Atrial Fibrillation Trial [CABANA]; NCT00911508).
Keywords: atrial fibrillation; catheter ablation; minority race; outcomes; randomized trials.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This work was supported by the National Institutes of Health (U01HL89709, U01HL089786, U01HL089907, and U01HL089645), St. Jude Medical Foundation and Corporation, Biosense Webster, Medtronic, and Boston Scientific Corporation. The content of this paper does not necessarily represent the views of the National Heart, Lung, and Blood Institute or the Department of Health and Human Services. Dr. Thomas has received grants from the National Heart, Lung, and Blood Institute (National Institutes of Health), Patient-Centered Outcomes Research Institute, and American Heart Association; and has received consulting fees from Sanofi, Boehringer Ingelheim, Janssen, Bristol Myers Squibb, and Medtronic during the conduct of the study. Dr. Al-Khalidi has received grants from the National Heart, Lung, and Blood Institute (National Institutes of Health) and the Mayo Clinic during the conduct of the study. Dr. Monahan has received grants from the National Heart, Lung, and Blood Institute (National Institutes of Health), St. Jude Foundation and Corporation, Biosense Webster, Medtronic, and Boston Scientific during the conduct of the study; has consulted without compensation from Biosense Webster; and has received personal fees from Thermedical outside the submitted work. Dr. Bahnson has received grants from the National Heart, Lung, and Blood Institute (National Institutes of Health) and the Mayo Clinic for conduct of the study; has received grants from Boston Scientific, St. Jude Medical Corporation, Biosense Webster, and Medtronic; and has received compensation for consulting from Cardiofocus and Ventrix during the conduct of the study but outside of the submitted work. Dr. Poole has received grants from ATriCure outside the submitted work. Dr. Mark has received grants from the National Heart, Lung, and Blood Institute (National Institutes of Health), the Mayo Clinic during the conduct of the study; and has received grants from Merck and HeartFlow outside the submitted work. Dr. Packer in the past 12 months has provided consulting services for Biosense Webster, Inc., Boston Scientific, CyberHeart, Medtronic, Inc., nContact, Sanofi, St. Jude Medical, and Toray Industries but has received no personal compensation for these consulting activities; has received grants from Abbott, Biosense Webster, Boston Scientific, CardioFocus, Medtronic, St. Jude Medical, CardioInsight, National Institutes of Health, Siemens, Thermedical, Endosense, Robertson Foundation, and Hansen Medical; has served on the advisory board without compensation for Abbott, Biosense Webster, Boston Scientific, CardioFocus, Medtronic, St. Jude Medical, Spectrum Dynamics, Siemens, Thermedical, Johnson & Johnson, and SigNum Preemptive Healthcare; has received speaking fees and honoraria from Biotronik and MediaSphere Medical; has received royalties from Wiley & Sons, Oxford, and St. Jude Medical; has joint equity with the Mayo Clinic in a privately held company, External Beam Ablation Medical Devices, outside the submitted work; and has received research funding from the NIH, Medtronic, Inc., Cryo Cath, Siemens AG, EP Limited, Minnesota Partnership for Biotechnology and Medical Genomics/University of Minnesota, Biosense Webster, Inc., and Boston Scientific. Mayo Clinic and Drs. Packer and Robb have a financial interest in mapping technology that may have been used at some of the 10 centers participating in this pilot research; in accordance with the Bayh-Dole Act, this technology has been licensed to St. Jude Medical, and Mayo Clinic and Drs. Packer and Robb received annual royalties >$10,000, the federal threshold for significant financial interest. Dr. Silverstein has reported that he has no relationships relevant to the contents of this paper to disclose.
Figures
Comment in
-
Catheter Ablation Is Better Than Drugs for Treatment of AF in Racial and Ethnic Minorities.J Am Coll Cardiol. 2021 Jul 13;78(2):139-141. doi: 10.1016/j.jacc.2021.05.008. J Am Coll Cardiol. 2021. PMID: 34238437 No abstract available.
-
Is Rhythm Control With Medication Unwittingly a Dangerous Proposition for Racial and Ethnic Minorities?J Am Coll Cardiol. 2021 Nov 9;78(19):e161. doi: 10.1016/j.jacc.2021.07.061. J Am Coll Cardiol. 2021. PMID: 34736572 No abstract available.
-
Racial and Ethnic Representation in Atrial Fibrillation Trials: CABANA and Beyond.J Am Coll Cardiol. 2021 Nov 9;78(19):e163-e164. doi: 10.1016/j.jacc.2021.08.054. J Am Coll Cardiol. 2021. PMID: 34736573 Free PMC article. No abstract available.
Similar articles
-
Effect of Catheter Ablation vs Antiarrhythmic Drug Therapy on Mortality, Stroke, Bleeding, and Cardiac Arrest Among Patients With Atrial Fibrillation: The CABANA Randomized Clinical Trial.JAMA. 2019 Apr 2;321(13):1261-1274. doi: 10.1001/jama.2019.0693. JAMA. 2019. PMID: 30874766 Free PMC article. Clinical Trial.
-
Recurrence of Atrial Fibrillation After Catheter Ablation or Antiarrhythmic Drug Therapy in the CABANA Trial.J Am Coll Cardiol. 2020 Jun 30;75(25):3105-3118. doi: 10.1016/j.jacc.2020.04.065. J Am Coll Cardiol. 2020. PMID: 32586583 Free PMC article. Clinical Trial.
-
Ablation Versus Drug Therapy for Atrial Fibrillation in Heart Failure: Results From the CABANA Trial.Circulation. 2021 Apr 6;143(14):1377-1390. doi: 10.1161/CIRCULATIONAHA.120.050991. Epub 2021 Feb 8. Circulation. 2021. PMID: 33554614 Free PMC article.
-
Catheter Ablation versus Antiarrhythmic Drug Therapy for Atrial Fibrillation (CABANA) Trial: Study Rationale and Design.Am Heart J. 2018 May;199:192-199. doi: 10.1016/j.ahj.2018.02.015. Epub 2018 Mar 7. Am Heart J. 2018. PMID: 29754661 Free PMC article. Review.
-
Catheter ablation for atrial fibrillation in heart failure with reduced ejection fraction: a systematic review and meta-analysis of randomized controlled trials.BMC Cardiovasc Disord. 2019 Jan 15;19(1):18. doi: 10.1186/s12872-019-0998-2. BMC Cardiovasc Disord. 2019. PMID: 30646857 Free PMC article.
Cited by
-
Effectiveness of Catheter Ablation in Left Ventricular Ejection Fraction, Stroke, Quality of Life, All-Cause Mortality, Sinus Rhythm Maintenance, and Hospitalization Rates as Compared to Medical Therapy.Cureus. 2023 Aug 12;15(8):e43372. doi: 10.7759/cureus.43372. eCollection 2023 Aug. Cureus. 2023. PMID: 37700942 Free PMC article. Review.
-
Atrial fibrillation: Primary prevention, secondary prevention, and prevention of thromboembolic complications: Part 2.Front Cardiovasc Med. 2023 Mar 10;9:1060096. doi: 10.3389/fcvm.2022.1060096. eCollection 2022. Front Cardiovasc Med. 2023. PMID: 36969508 Free PMC article. Review.
-
Performance of the novel ANTWERP score in predicting heart function improvement after atrial fibrillation ablation in Asian patients with heart failure.J Arrhythm. 2024 Oct 18;40(6):1359-1369. doi: 10.1002/joa3.13162. eCollection 2024 Dec. J Arrhythm. 2024. PMID: 39669923 Free PMC article.
-
Racial Disparity in Referral for Catheter Ablation for Atrial Fibrillation at a Single Integrated Health System.J Am Heart Assoc. 2022 Sep 20;11(18):e025831. doi: 10.1161/JAHA.122.025831. Epub 2022 Sep 8. J Am Heart Assoc. 2022. PMID: 36073632 Free PMC article.
-
Atrial Fibrillation: The Year of 2021 in Review.J Innov Card Rhythm Manag. 2022 Jan 15;13(1):4847-4851. doi: 10.19102/icrm.2022.130108. eCollection 2022 Jan. J Innov Card Rhythm Manag. 2022. PMID: 35127238 Free PMC article. No abstract available.
References
-
- Calkins H, Hindricks G, Cappato R et al.2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation: Executive summary. Heart Rhythm 2017;14:e445–e494. - PubMed
-
- Leef GC, Perino AC, Cluckey A et al.Geographic and racial representation and reported success rates of studies of catheter ablation for atrial fibrillation: Findings from the SMASH-AF meta-analysis study cohort. J Cardiovasc Electrophysiol 2018;29:747–755. - PubMed
-
- Hoyt H, Nazarian S, Alhumaid F et al.Demographic profile of patients undergoing catheter ablation of atrial fibrillation. J Cardiovasc Electrophysiol 2011;22:994–8. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
