

Association of early positive end-expiratory pressure settings with ventilator-free days in patients with coronavirus disease 2019 acute respiratory distress syndrome: A secondary analysis of the Practice of VENTilation in COVID-19 study
- PMID: 34238782
- PMCID: PMC8630930
- DOI: 10.1097/EJA.0000000000001565
Association of early positive end-expiratory pressure settings with ventilator-free days in patients with coronavirus disease 2019 acute respiratory distress syndrome: A secondary analysis of the Practice of VENTilation in COVID-19 study
Abstract
Background: There is uncertainty about how much positive end-expiratory pressure (PEEP) should be used in patients with acute respiratory distress syndrome (ARDS) due to coronavirus disease 2019 (COVID-19).
Objective: To investigate whether a higher PEEP strategy is superior to a lower PEEP strategy regarding the number of ventilator-free days (VFDs).
Design: Multicentre observational study conducted from 1 March to 1 June 2020.
Setting and patients: Twenty-two ICUs in The Netherlands and 933 invasively ventilated COVID-19 ARDS patients.
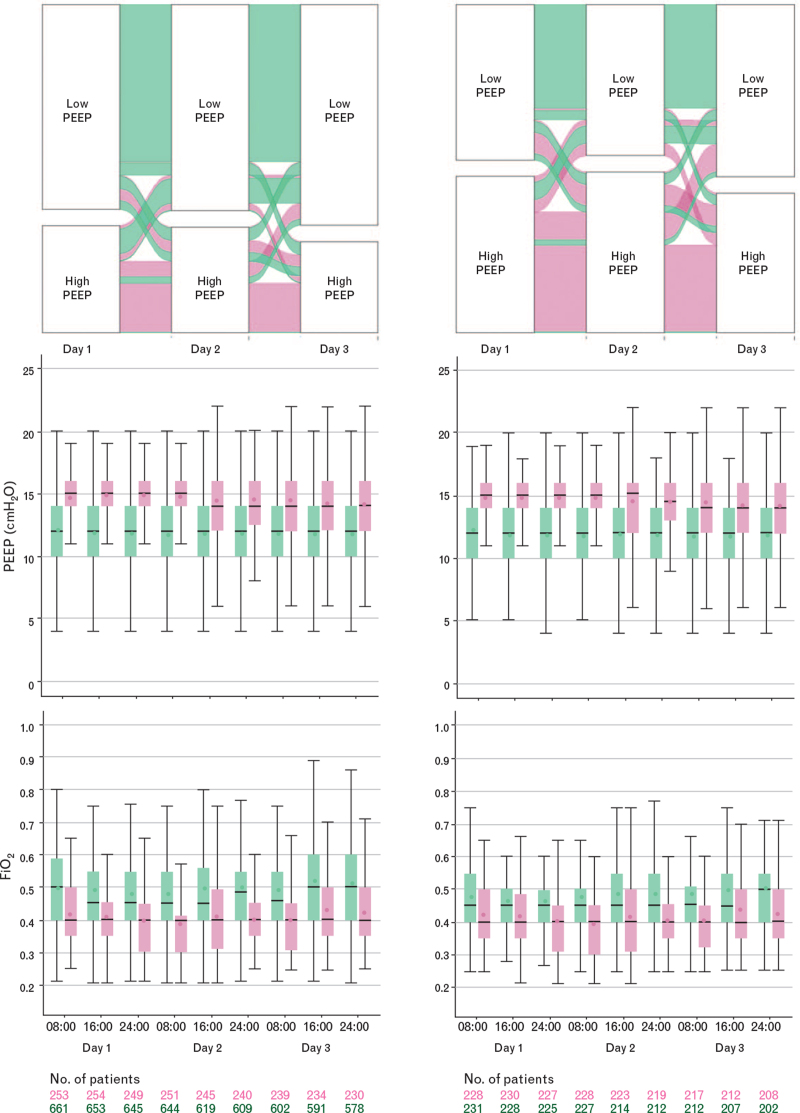
Interventions: Patients were categorised retrospectively as having received invasive ventilation with higher (n=259) or lower PEEP (n=674), based on the high and low PEEP/FiO2 tables of the ARDS Network, and using ventilator settings and parameters in the first hour of invasive ventilation, and every 8 h thereafter at fixed time points during the first four calendar days. We also used propensity score matching to control for observed confounding factors that might influence outcomes.
Main outcomes and measures: The primary outcome was the number of VFDs. Secondary outcomes included distant organ failures including acute kidney injury (AKI) and use of renal replacement therapy (RRT), and mortality.
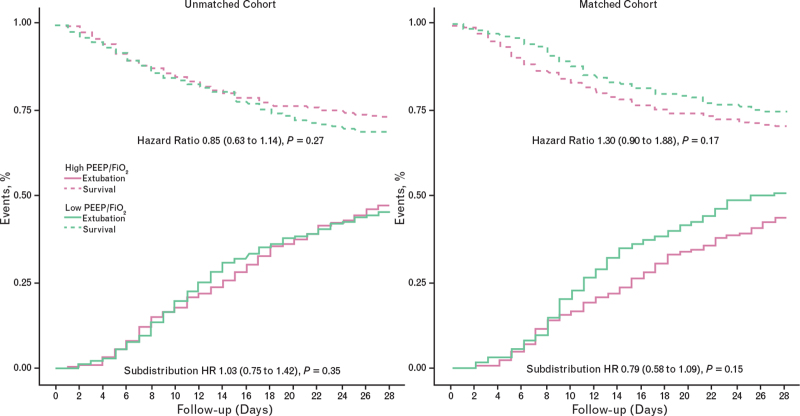
Results: In the unmatched cohort, the higher PEEP strategy had no association with the median [IQR] number of VFDs (2.0 [0.0 to 15.0] vs. 0.0 [0.0 to 16.0] days). The median (95% confidence interval) difference was 0.21 (-3.34 to 3.78) days, P = 0.905. In the matched cohort, the higher PEEP group had an association with a lower median number of VFDs (0.0 [0.0 to 14.0] vs. 6.0 [0.0 to 17.0] days) a median difference of -4.65 (-8.92 to -0.39) days, P = 0.032. The higher PEEP strategy had associations with higher incidence of AKI (in the matched cohort) and more use of RRT (in the unmatched and matched cohorts). The higher PEEP strategy had no association with mortality.
Conclusion: In COVID-19 ARDS, use of higher PEEP may be associated with a lower number of VFDs, and may increase the incidence of AKI and need for RRT.
Trial registration: Practice of VENTilation in COVID-19 is registered at ClinicalTrials.gov, NCT04346342.
Copyright © 2021 European Society of Anaesthesiology and Intensive Care. Unauthorized reproduction of this article is prohibited.
Conflict of interest statement
Subdistribution hazard ratio from a clustered Fine–Gray competing risk model, with death before extubation treated as competing risk.
Hazard ratio from a (shared-frailty) Cox proportional hazard model. For the ICU and hospital length of stay analyses, all patients who died prior to discharge were assigned the maximum length of stay to account for death as a competing risk in this model.
Figures
References
-
- Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med 2014; 370:980. - PubMed
-
- Brower RG, Matthay MA, Morris A, et al. . Acute Respiratory Distress Syndrome Network. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med 2000; 342:1301–1308. - PubMed
-
- Mercat A, Richard JC, Vielle B, et al. . Positive end-expiratory pressure setting in adults with acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2008; 299:646–655. - PubMed
-
- Meade MO, Cook DJ, Guyatt GH, et al. . Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA 2008; 299:637–645. - PubMed
-
- Cavalcanti AB, Suzumura EA, Laranjeira LN, et al. . Writing Group for the Alveolar Recruitment for Acute Respiratory Distress Syndrome Trial I. Effect of lung recruitment and titrated positive end-expiratory pressure (PEEP) vs low PEEP on mortality in patients with acute respiratory distress syndrome: a randomized clinical trial. JAMA 2017; 318:1335–1345. - PMC - PubMed
