

Colorectal cancer incidence and mortality: the current status, temporal trends and their attributable risk factors in 60 countries in 2000-2019
- PMID: 34238851
- PMCID: PMC8382382
- DOI: 10.1097/CM9.0000000000001619
Colorectal cancer incidence and mortality: the current status, temporal trends and their attributable risk factors in 60 countries in 2000-2019
Abstract
Background: Globally, colorectal cancer (CRC) imposes a substantial burden on healthcare systems and confers considerable medical expenditures. We aimed to evaluate the global and regional burden in epidemiological trends and factors associated with the incidence and mortality of CRC.
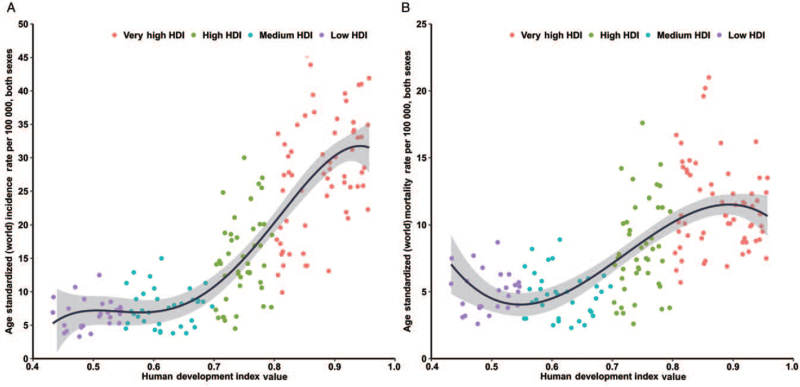
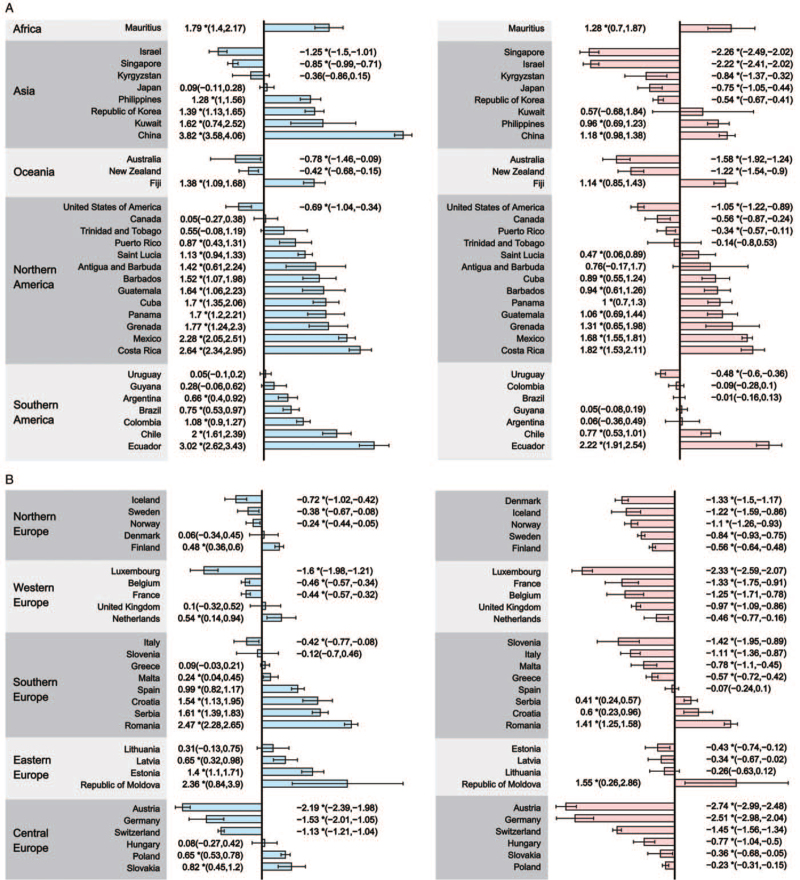
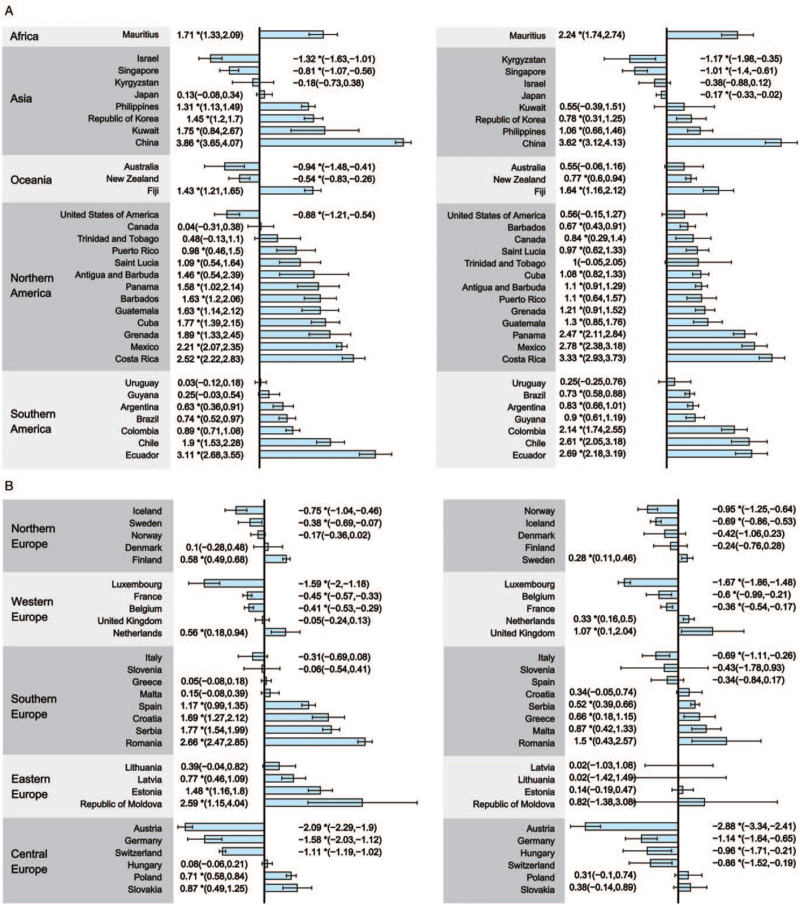
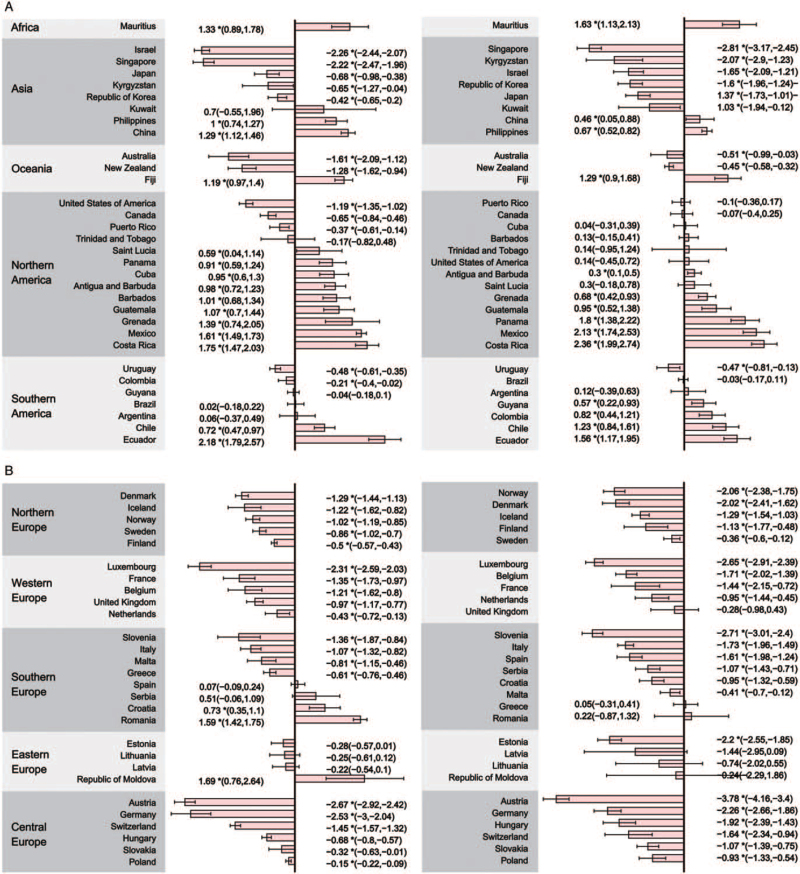
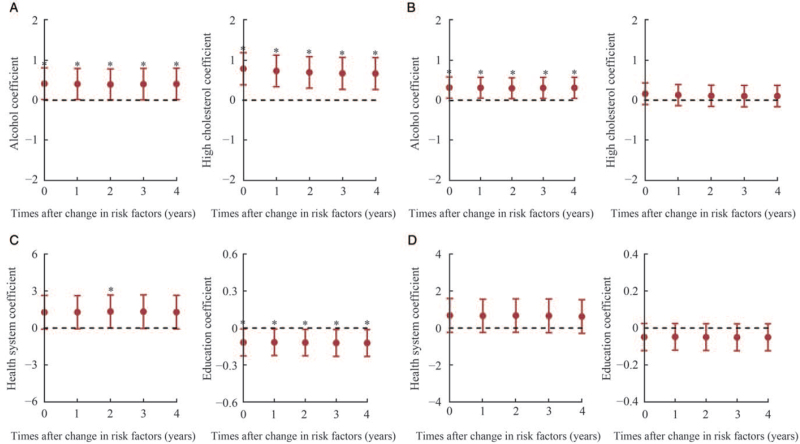
Methods: We used data from the GLOBOCAN database to estimate CRC incidence and mortality worldwide in 2020 and their association with the human development index (HDI). Trends of age-standardized rates of incidence and mortality in 60 countries (2000-2019) were evaluated by Joinpoint regression analysis using data of Global Burden of Disease 2019. The association between exposure to country-level lifestyle, metabolic and socioeconomic factors obtained from the World Health Organization Global Health Observatory and World Bank DataBank data and CRC incidence and mortality was determined by multivariable linear regression.
Results: CRC incidence and mortality varied greatly in the 60 selected countries, and much higher incidence and mortality were observed in countries with higher HDIs, and vice versa. From 2000 to 2019, significant increases of incidence and mortality were observed for 33 countries (average annual percent changes [AAPCs], 0.24-3.82) and 18 countries (AAPCs, 0.41-2.22), respectively. A stronger increase in incidence was observed among males (AAPCs, 0.36-4.54) and individuals <50 years (AAPCs, 0.56-3.86). Notably, 15 countries showed significant decreases in both incidence (AAPCs, -0.24 to -2.19) and mortality (AAPCs, -0.84 to -2.74). A significant increase of incidence among individuals <50 years was observed in 30 countries (AAPCs, 0.28-3.62). Countries with higher incidence were more likely to have a higher prevalence of alcohol drinking, higher level of cholesterol level, higher level of unemployment, and a poorer healthcare system.
Conclusions: Some high-HDI countries showed decreasing trends in CRC incidence and mortality, whereas developing countries that previously had low disease burden showed significantly increased incidence and mortality trends, especially in males and populations ≥50 years, which require targeted preventive health programs.
Copyright © 2021 The Chinese Medical Association, produced by Wolters Kluwer, Inc. under the CC-BY-NC-ND license.
Conflict of interest statement
None.
Figures
References
-
- Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. . Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71:209–249. doi: 10.3322/caac.21660. - PubMed
-
- Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017; 66:683–691. doi: 10.1136/gutjnl-2015-310912. - PubMed
-
- Händel MN, Rohde JF, Jacobsen R, Nielsen SM, Christensen R, Alexander DD, et al. . Processed meat intake and incidence of colorectal cancer: a systematic review and meta-analysis of prospective observational studies. Eur J Clin Nutr 2020; 74:1132–1148. doi: 10.1038/s41430-020-0576-9. - PubMed
-
- Cheng J, Chen Y, Wang X, Wang J, Yan Z, Gong G, et al. . Meta-analysis of prospective cohort studies of cigarette smoking and the incidence of colon and rectal cancers. Eur J Cancer Prev 2015; 24:6–15. doi: 10.1097/cej.0000000000000011. - PubMed
-
- Botteri E, Iodice S, Bagnardi V, Raimondi S, Lowenfels AB, Maisonneuve P. Smoking and colorectal cancer: a meta-analysis. JAMA 2008; 300:2765–2778. doi: 10.1001/jama.2008.839. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
