

Comparison of Risk Factors, Safety, and Efficacy Outcomes of Mechanical Thrombectomy in Posterior vs. Anterior Circulation Large Vessel Occlusion
- PMID: 34239498
- PMCID: PMC8258169
- DOI: 10.3389/fneur.2021.687134
Comparison of Risk Factors, Safety, and Efficacy Outcomes of Mechanical Thrombectomy in Posterior vs. Anterior Circulation Large Vessel Occlusion
Abstract
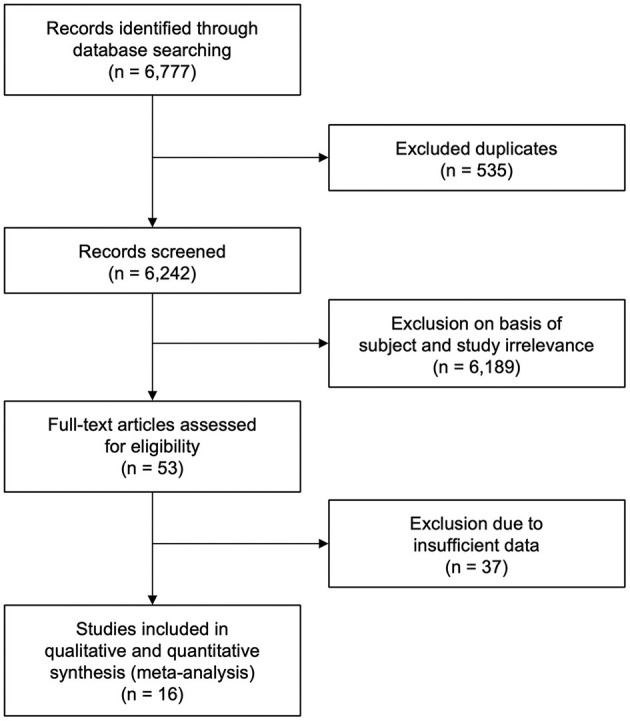
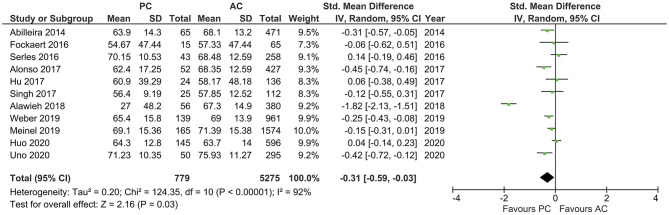
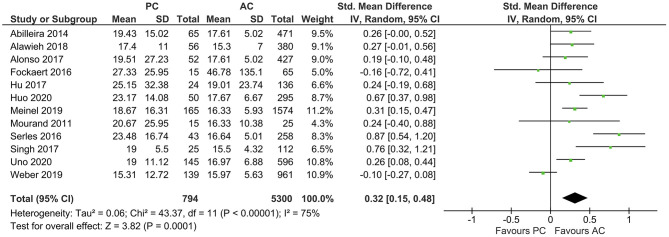
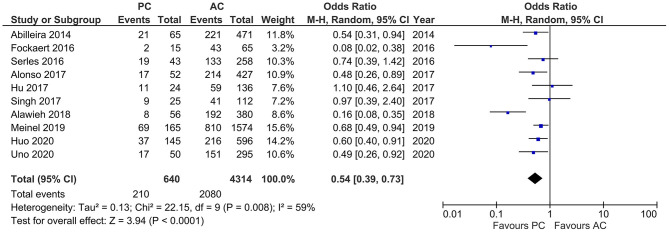
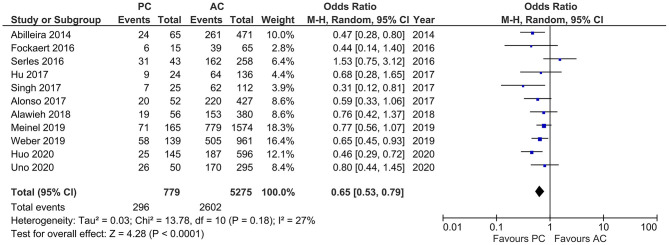
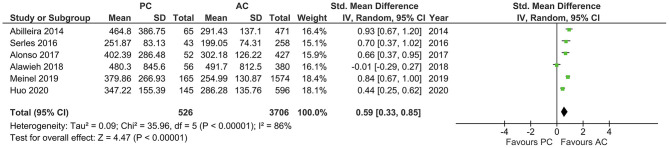
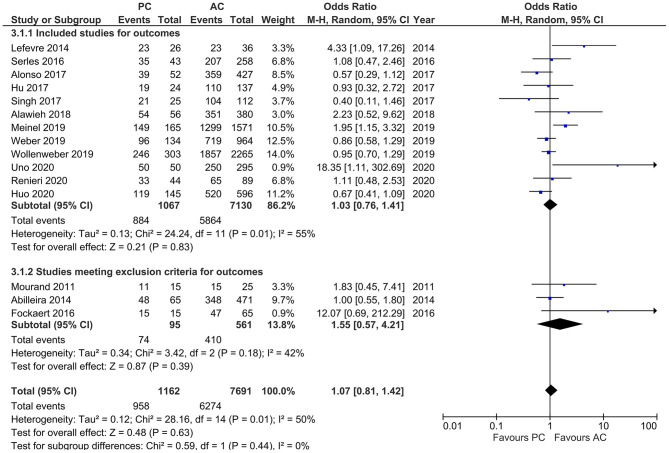
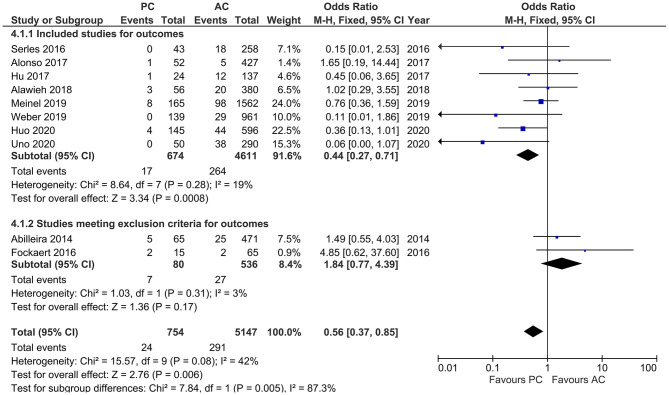
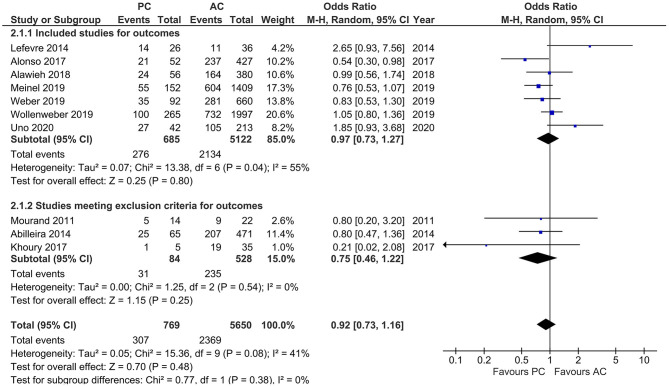
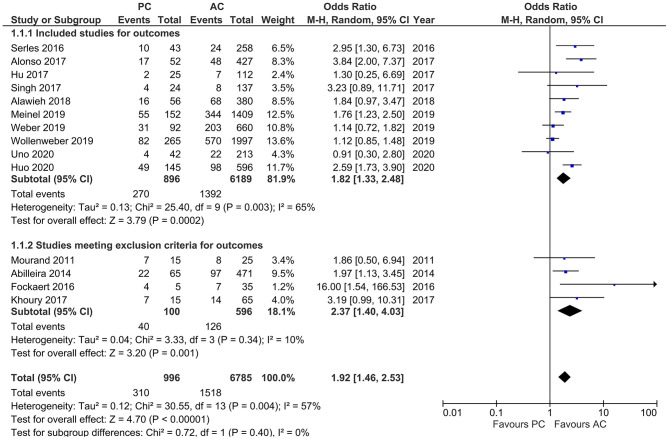
Background and Purpose: It is believed that stroke occurring due to posterior circulation large vessel occlusion (PCLVO) and that occurring due to anterior circulation large vessel occlusion (ACLVO) differ in terms of their pathophysiology and the outcome of their acute management in relation to endovascular mechanical thrombectomy (MT). Limited sample size and few randomized controlled trials (RCTs) with respect to PCLVO make the safety and efficacy of MT, which has been confirmed in ACLVO, difficult to assess in the posterior circulation. We therefore conducted a meta-analysis to study to which extent MT in PCLVO differs from ACLVO. Materials and Methods: We searched the databases PubMed, Cochrane, and EMBASE for studies published between 2010 and January 2021, with information on risk factors, safety, and efficacy outcomes of MT in PCLVO vs. ACLVO and conducted a systematic review and meta-analysis; we compared baseline characteristics, reperfusion treatment profiles [including rates of intravenous thrombolysis (IVT) and onset-to-IVT and onset-to-groin puncture times], recanalization success [Thrombolysis In Cerebral Infarction scale (TICI) 2b/3], symptomatic intracranial hemorrhage (sICH), and favorable functional outcome [modified Rankin Score (mRS) 0-2] and mortality at 90 days. Results: Sixteen studies with MT PCLVO (1,172 patients) and ACLVO (7,726 patients) were obtained from the search. The pooled estimates showed higher baseline National Institutes of Health Stroke Scale (NIHSS) score (SMD 0.32, 95% CI 0.15-0.48) in the PCLVO group. PCLVO patients received less often IVT (OR 0.65, 95% CI 0.53-0.79). Onset-to-IVT time (SMD 0.86, 95% CI 0.45-1.26) and onset-to-groin puncture time (SMD 0.59, 95% CI 0.33-0.85) were longer in the PCLVO group. The likelihood of obtaining successful recanalization and favorable functional outcome at 90 days was comparable between the two groups. PCLVO was, however, associated with less sICH (OR 0.56, 95% CI 0.37-0.85) but higher mortality (OR 1.92, 95% CI 1.46-2.53). Conclusions: This meta-analysis indicates that MT in PCLVO may be comparably efficient in obtaining successful recanalization and 90 day favorable functional outcome just as in ACLVO. Less sICH in MT-treated PCLVO patients might be the result of the lower IVT rate in this group. Higher baseline NIHSS and longer onset-to-IVT and onset-to-groin puncture times may have contributed to a higher 90 day mortality in PCLVO patients.
Keywords: Ischemic Stroke; Large Vessel Occlusion; Mechanical Thrombectomy/Endovascular treatment; acute ischemic stroke; anterior circulation; endovascular stroke treatment; endovascular thrombectomy; large vessel occlusion; mechanical thrombectomy; posterior circulation.
Copyright © 2021 Mbroh, Poli, Tünnerhoff, Gomez-Exposito, Wang, Bender, Hempel, Hennersdorf, Feil, Mengel, Ziemann and Poli.
Conflict of interest statement
UZ received research grants from BMS, European Research Council, German Federal Ministry of Education and Research, German Research Foundation, Janssen Pharmaceuticals, and Takeda, and personal consulting fees from Bayer, CorTec, and Pfizer. SP received research grants from BMS/Pfizer, Daiichi Sankyo, European Union, German Federal Joint Committee Innovation Fund, and German Federal Ministry of Education and Research, and speakers' honoraria/consulting fees from AstraZeneca, Bayer, Boehringer-Ingelheim, BMS/Pfizer, Daiichi Sankyo, Portola, and Werfen. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

References
-
- Nogueira RG, Lutsep HL, Gupta R, Jovin TG, Albers GW, Walker GA, et al. . Trevo versus Merci retrievers for thrombectomy revascularisation of large vessel occlusions in acute ischaemic stroke (TREVO 2): a randomised trial. Lancet. (2012) 380:1231–40. 10.1016/S0140-6736(12)61299-9 - DOI - PMC - PubMed
-
- Saver JL, Jahan R, Levy EI, Jovin TG, Baxter B, Nogueira RG, et al. . Solitaire flow restoration device versus the Merci Retriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet. (2012) 380:1241–9. 10.1016/S0140-6736(12)61384-1 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources