

International retrospective natural history study of LMNA-related congenital muscular dystrophy
- PMID: 34240052
- PMCID: PMC8260964
- DOI: 10.1093/braincomms/fcab075
International retrospective natural history study of LMNA-related congenital muscular dystrophy
Abstract
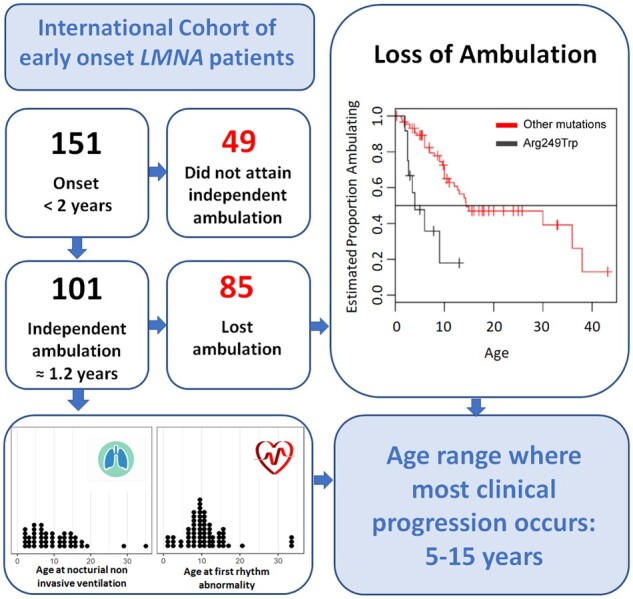
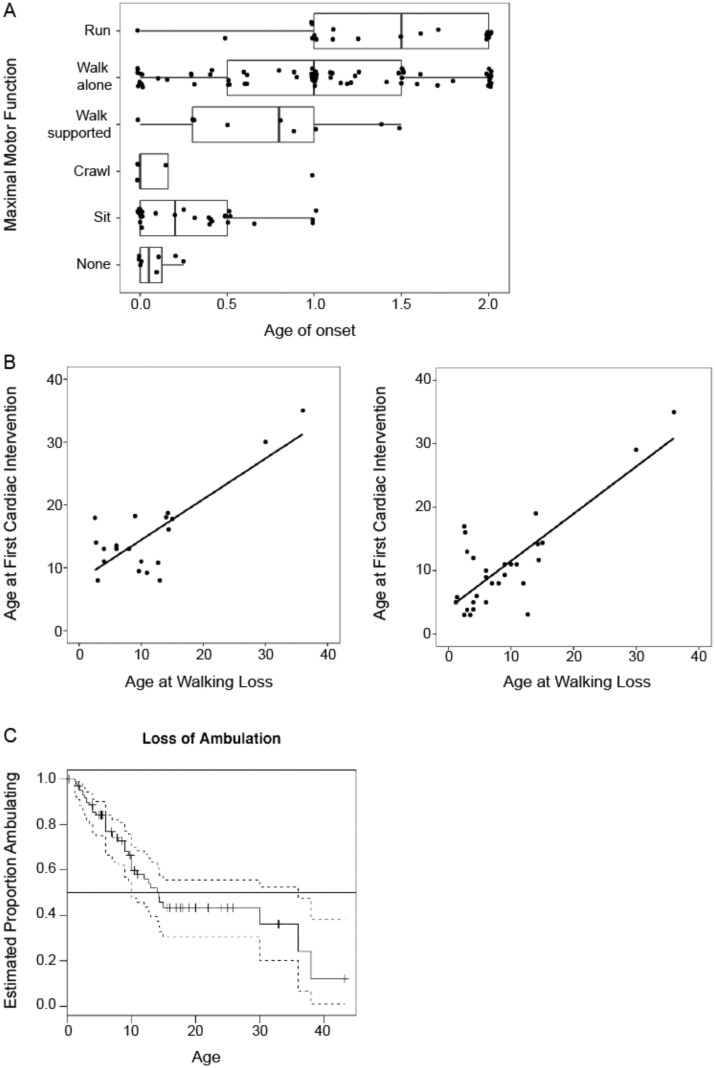
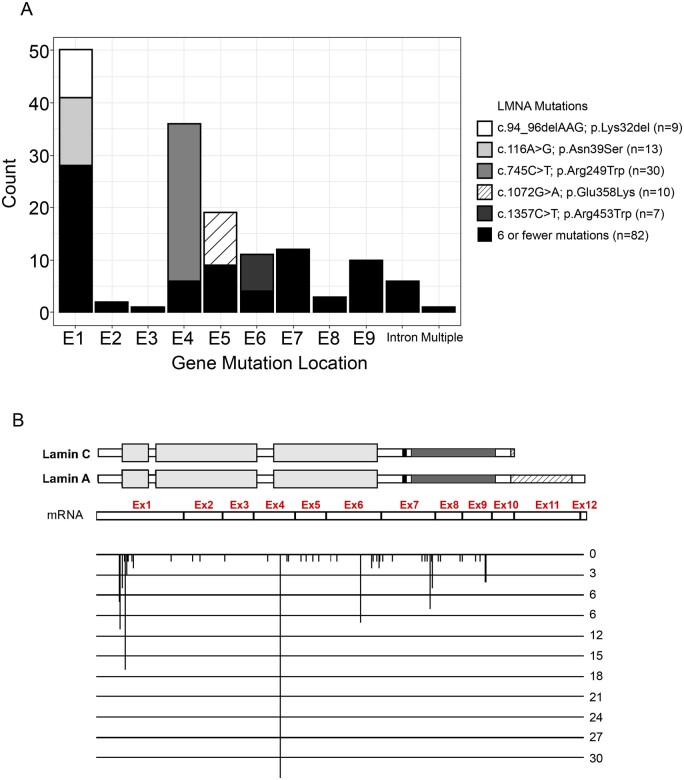
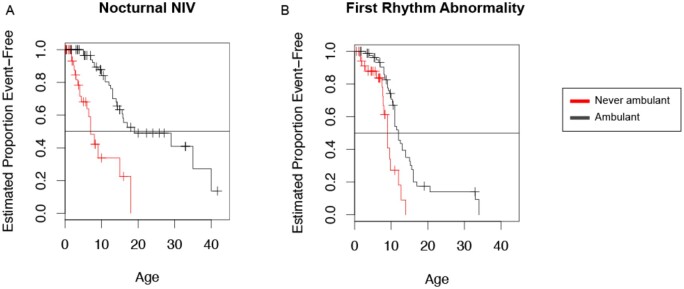
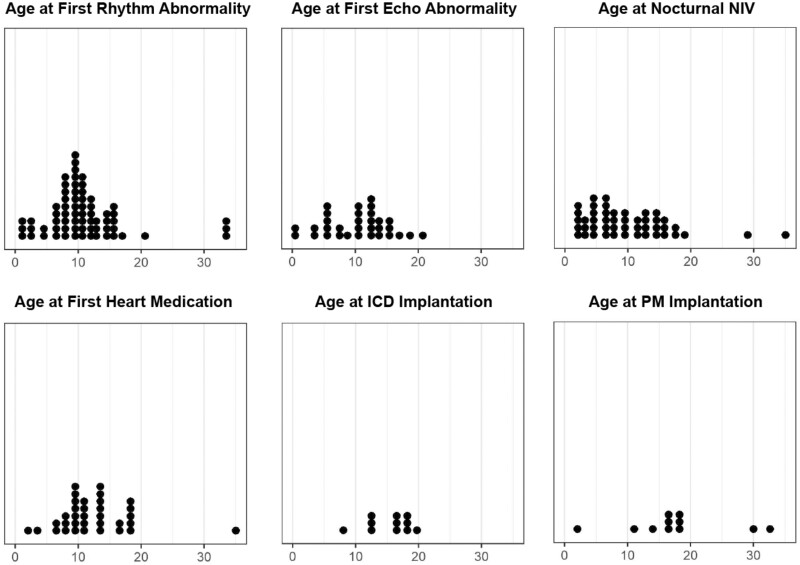
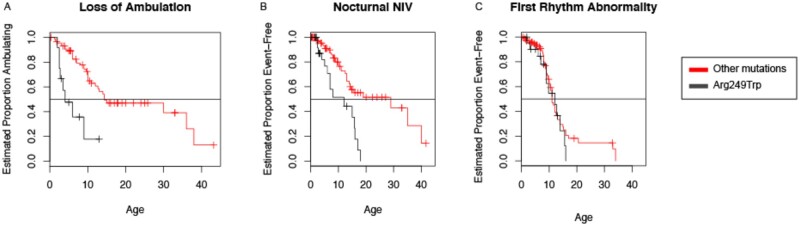
Muscular dystrophies due to heterozygous pathogenic variants in LMNA gene cover a broad spectrum of clinical presentations and severity with an age of onset ranging from the neonatal period to adulthood. The natural history of these conditions is not well defined, particularly in patients with congenital or early onset who arguably present with the highest disease burden. Thus the definition of natural history endpoints along with clinically revelant outcome measures is essential to establishing both clinical care planning and clinical trial readiness for this patient group. We designed a large international cross-sectional retrospective natural history study of patients with genetically proven muscle laminopathy who presented with symptoms before two years of age intending to identify and characterize an optimal clinical trial cohort with pertinent motor, cardiac and respiratory endpoints. Quantitative statistics were used to evaluate associations between LMNA variants and distinct clinical events. The study included 151 patients (median age at symptom onset 0.9 years, range: 0.0-2.0). Age of onset and age of death were significantly lower in patients who never acquired independent ambulation compared to patients who achieved independent ambulation. Most of the patients acquired independent ambulation (n = 101, 66.9%), and subsequently lost this ability (n = 86; 85%). The age of ambulation acquisition (median: 1.2 years, range: 0.8-4.0) and age of ambulation loss (median: 7 years, range: 1.2-38.0) were significantly associated with the age of the first respiratory interventions and the first cardiac symptoms. Respiratory and gastrointestinal interventions occurred during first decade while cardiac interventions occurred later. Genotype-phenotype analysis showed that the most common mutation, p.Arg249Trp (20%), was significantly associated with a more severe disease course. This retrospective natural history study of early onset LMNA-related muscular dystrophy confirms the progressive nature of the disorder, initially involving motor symptoms prior to onset of other symptoms (respiratory, orthopaedic, cardiac and gastrointestinal). The study also identifies subgroups of patients with a range of long-term outcomes. Ambulatory status was an important mean of stratification along with the presence or absence of the p.Arg249Trp mutation. These categorizations will be important for future clinical trial cohorts. Finally, this study furthers our understanding of the progression of early onset LMNA-related muscular dystrophy and provides important insights into the anticipatory care needs of LMNA-related respiratory and cardiac manifestations.
Keywords: LMNA; early onset; laminopathies; muscular dystrophy; striated muscle.
© The Author(s) (2021). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Macquart C, Ben Yaou R, Muchir A, Wahbi K., Bonne G.. Clinical features and therapeutic strategies for managing the striated muscle laminopathies. Expert Opin Orphan D. 2016;4:631–638.
-
- Bonne G, Di Barletta MR, Varnous S, et al.Mutations in the gene encoding lamin A/C cause autosomal dominant Emery–Dreifuss muscular dystrophy. Nat Genet. 1999;21:285–288. - PubMed
-
- Fatkin D, MacRae C, Sasaki T, et al.Missense mutations in the rod domain of the lamin A/C gene as causes of dilated cardiomyopathy and conduction-system disease. N Engl J Med. 1999;341:1715–1724. - PubMed
-
- Muchir A, Bonne G, van der Kooi AJ, et al.Identification of mutations in the gene encoding lamins A/C in autosomal dominant limb girdle muscular dystrophy with atrioventricular conduction disturbances (LGMD1B). Hum Mol Genet. 2000;9:1453–1459. - PubMed
-
- Bonne G, Mercuri E, Muchir A, et al.Clinical and molecular genetic spectrum of autosomal dominant Emery–Dreifuss muscular dystrophy due to mutations of the lamin A/C gene. Ann Neurol. 2000;48:170–180. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous