

Prevalence of nodal involvement in rectal cancer after chemoradiotherapy
- PMID: 34240110
- PMCID: PMC8604154
- DOI: 10.1093/bjs/znab194
Prevalence of nodal involvement in rectal cancer after chemoradiotherapy
Abstract
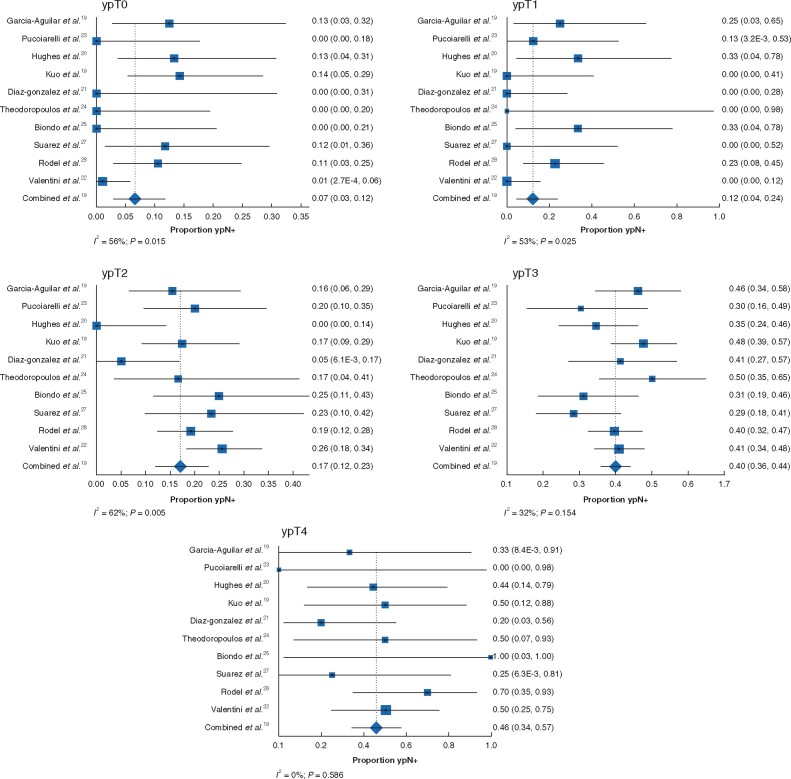
Background: The purpose of this study was to investigate the prevalence of ypN+ status according to ypT category in patients with locally advanced rectal cancer treated with chemoradiotherapy and total mesorectal excision, and to assess the impact of ypN+ on disease recurrence and survival by pooled analysis of individual-patient data.
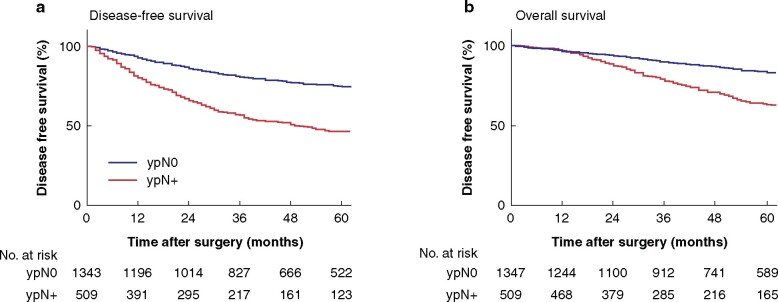
Methods: Individual-patient data from 10 studies of chemoradiotherapy for rectal cancer were included. Pooled rates of ypN+ disease were calculated with 95 per cent confidence interval for each ypT category. Kaplan-Meier and Cox regression analyses were undertaken to assess influence of ypN status on 5-year disease-free survival (DFS) and overall survival (OS).
Results: Data on 1898 patients were included in the study. Median follow-up was 50 (range 0-219) months. The pooled rate of ypN+ disease was 7 per cent for ypT0, 12 per cent for ypT1, 17 per cent for ypT2, 40 per cent for ypT3, and 46 per cent for ypT4 tumours. Patients with ypN+ disease had lower 5-year DFS and OS (46.2 and 63.4 per cent respectively) than patients with ypN0 tumours (74.5 and 83.2 per cent) (P < 0.001). Cox regression analyses showed ypN+ status to be an independent predictor of recurrence and death.
Conclusion: Risk of nodal metastases (ypN+) after chemoradiotherapy increases with advancing ypT category and needs to be considered if an organ-preserving strategy is contemplated.
Plain language summary
When patients are diagnosed with rectal cancer and the tumour grows beyond the rectal wall there is a high risk that the tumour has spread to nearby lymph nodes. This study showed that this relationship between tumour invasion depth and lymph node involvement is similar after treatment with (chemo)radiotherapy. Patients who have tumour cells remaining in the lymph nodes after (chemo) radiotherapy have a worse prognosis than patients who do not have cancer cells remaining in the lymph nodes. When an organ-preserving treatment is considered as an alternative therapy, this should be kept in mind during patient counselling.
© The Author(s) 2021. Published by Oxford University Press on behalf of BJS Society Ltd. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986;1:1479–1482 - PubMed
-
- Sauer R, Becker H, Hohenberger W, Rödel C, Wittekind C, Fietkau R et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351:1731–1740 - PubMed
-
- van der Valk MJM, Hilling DE, Bastiaannet E, Meershoek-Klein Kranenbarg E, Beets GL, Figueiredo NL et al. Long-term outcomes of clinical complete responders after neoadjuvant treatment for rectal cancer in the International Watch & Wait Database (IWWD): an international multicentre registry study. Lancet 2018;391:2537–2545 - PubMed
-
- Dossa F, Chesney TR, Acuna SA, Baxter NN. A watch-and-wait approach for locally advanced rectal cancer after a clinical complete response following neoadjuvant chemoradiation: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol 2017;2:501–513 - PubMed
-
- Dattani M, Heald RJ, Goussous G, Broadhurst J, Sao JG, Habr-Gama A. Oncological and survival outcomes in watch and wait patients with a clinical complete response after neoadjuvant chemoradiotherapy for rectal cancer: a systematic review and pooled analysis. Ann Surg 2018;268:955–967 - PubMed
