

Pulsed field ablation prevents chronic atrial fibrotic changes and restrictive mechanics after catheter ablation for atrial fibrillation
- PMID: 34240134
- PMCID: PMC8576285
- DOI: 10.1093/europace/euab155
Pulsed field ablation prevents chronic atrial fibrotic changes and restrictive mechanics after catheter ablation for atrial fibrillation
Abstract
Aims: Pulsed field ablation (PFA), a non-thermal ablative modality, may show different effects on the myocardial tissue compared to thermal ablation. Thus, this study aimed to compare the left atrial (LA) structural and mechanical characteristics after PFA vs. thermal ablation.
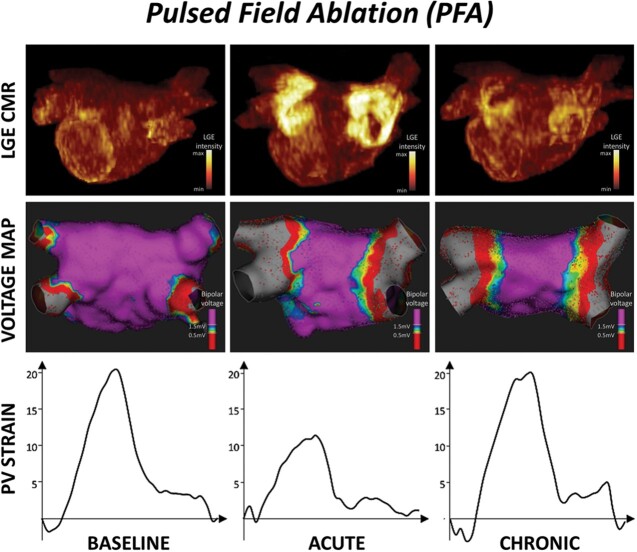
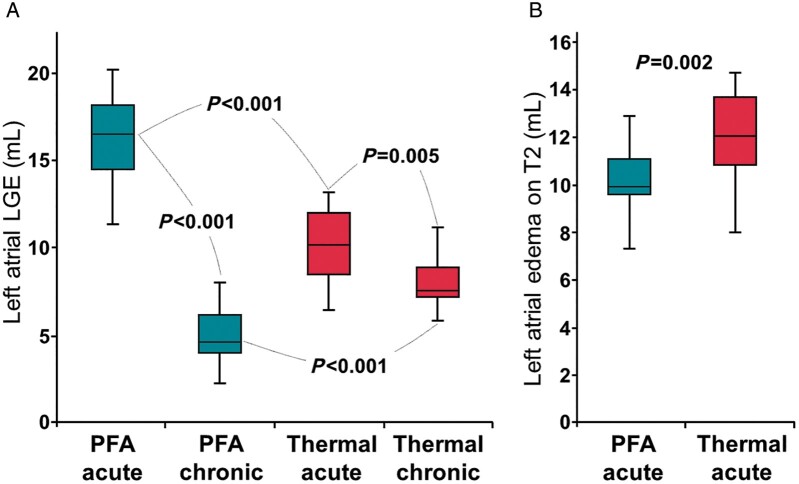
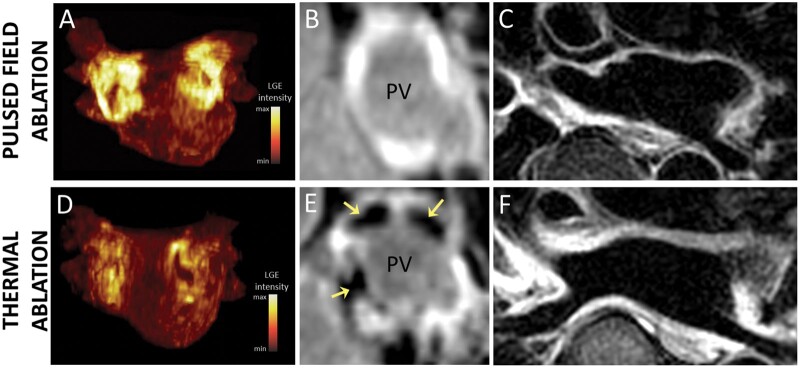
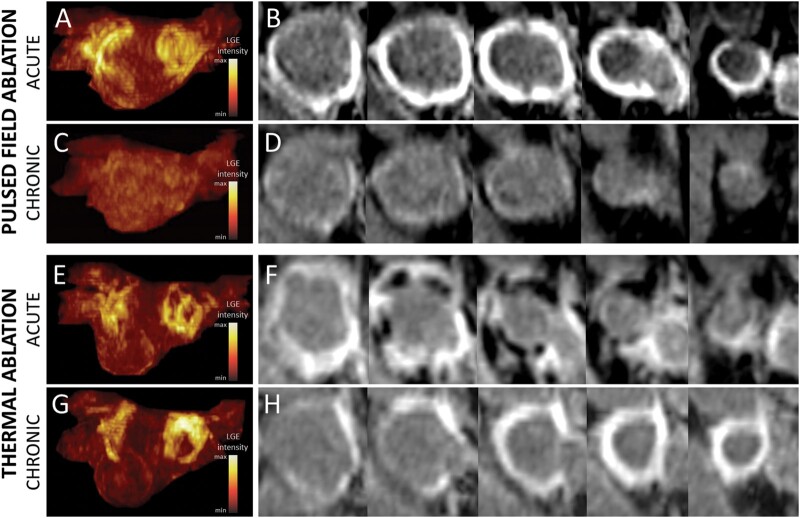
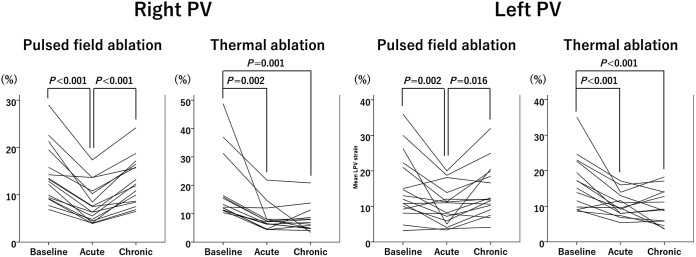
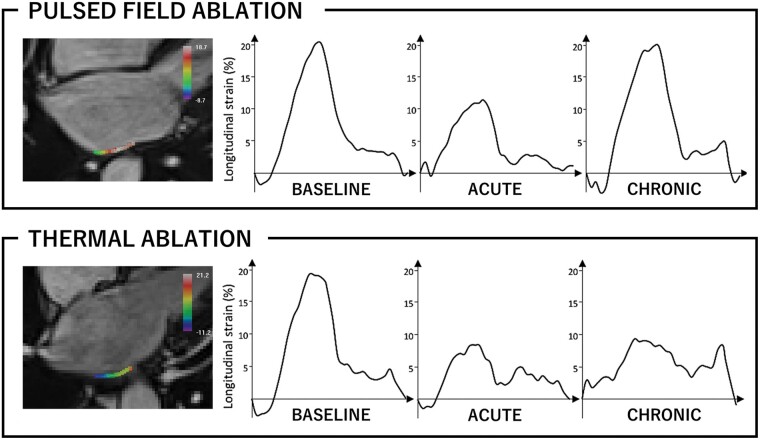
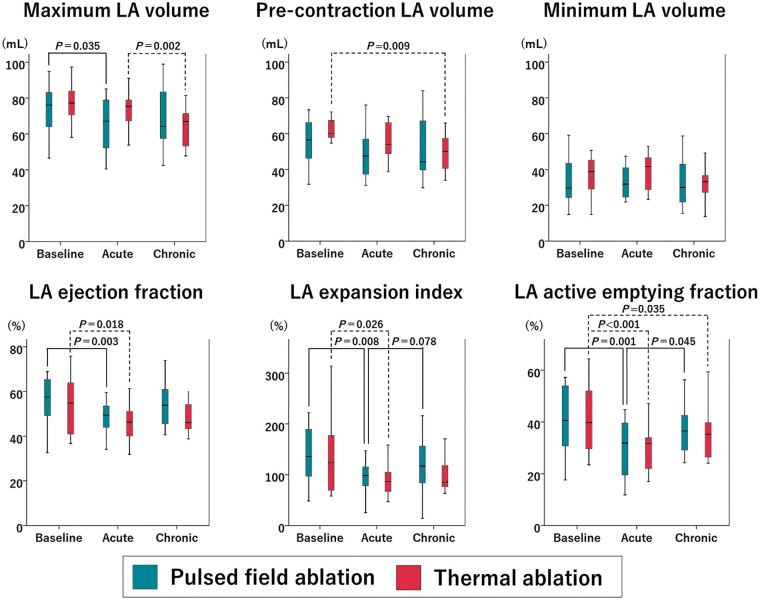
Methods and results: Cardiac magnetic resonance was performed pre-ablation, acutely (<3 h), and 3 months post-ablation in 41 patients with paroxysmal atrial fibrillation (AF) undergoing pulmonary vein (PV) isolation with PFA (n = 18) or thermal ablation (n = 23, 16 radiofrequency ablations, 7 cryoablations). Late gadolinium enhancement (LGE), T2-weighted, and cine images were analysed. In the acute stage, LGE volume was 60% larger after PFA vs. thermal ablation (P < 0.001), and oedema on T2 imaging was 20% smaller (P = 0.002). Tissue changes were more homogeneous after PFA than after thermal ablation, with no sign of microvascular damage or intramural haemorrhage. In the chronic stage, the majority of acute LGE had disappeared after PFA, whereas most LGE persisted after thermal ablation. The maximum strain on PV antra, the LA expansion index, and LA active emptying fraction declined acutely after both PFA and thermal ablation but recovered at the chronic stage only with PFA.
Conclusion: Pulsed field ablation induces large acute LGE without microvascular damage or intramural haemorrhage. Most LGE lesions disappear in the chronic stage, suggesting a specific reparative process involving less chronic fibrosis. This process may contribute to a preserved tissue compliance and LA reservoir and booster pump functions.
Keywords: Atrial fibrillation; Atrial fibrosis; Cardiac magnetic resonance; Catheter ablation; Pulsed field ablation.
© The Author(s) 2021. Published by Oxford University Press on behalf of the European Society of Cardiology.
Figures
Comment in
-
Pulsed field ablation: have we finally found the holy grail?Europace. 2021 Nov 8;23(11):1691-1692. doi: 10.1093/europace/euab169. Europace. 2021. PMID: 34245276 No abstract available.
References
-
- de Gouveia RH, Melo J, Santiago T, Martins AP.. Comparison of the healing mechanisms of myocardial lesions induced by dry radiofrequency and microwave epicardial ablation. Pacing Clin Electrophysiol 2006;29:278–82. - PubMed
-
- Cochet H, Scherr D, Zellerhoff S, Sacher F, Derval N, Denis A. et al. Atrial structure and function 5 years after successful ablation for persistent atrial fibrillation: an MRI study. J Cardiovasc Electrophysiol 2014;25:671–9. - PubMed
-
- Kato R, Lickfett L, Meininger G, Dickfeld T, Wu R, Juang G. et al. Pulmonary vein anatomy in patients undergoing catheter ablation of atrial fibrillation: lessons learned by use of magnetic resonance imaging. Circulation 2003;107:2004–10. - PubMed
-
- Gibson DN, Di Biase L, Mohanty P, Patel JD, Bai R, Sanchez J. et al. Stiff left atrial syndrome after catheter ablation for atrial fibrillation: clinical characterization, prevalence, and predictors. Heart Rhythm 2011;8:1364–71. - PubMed
-
- Davalos RV, Mir IL, Rubinsky B.. Tissue ablation with irreversible electroporation. Ann Biomed Eng 2005;33:223–31. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
