

Brain growth after surgical treatment for infant postinfectious hydrocephalus in Sub-Saharan Africa: 2-year results of a randomized trial
- PMID: 34243157
- PMCID: PMC8742836
- DOI: 10.3171/2021.2.PEDS20949
Brain growth after surgical treatment for infant postinfectious hydrocephalus in Sub-Saharan Africa: 2-year results of a randomized trial
Abstract
Objective: Hydrocephalus in infants, particularly that with a postinfectious etiology, is a major public health burden in Sub-Saharan Africa. The authors of this study aimed to determine whether surgical treatment of infant postinfectious hydrocephalus in Uganda results in sustained, long-term brain growth and improved cognitive outcome.
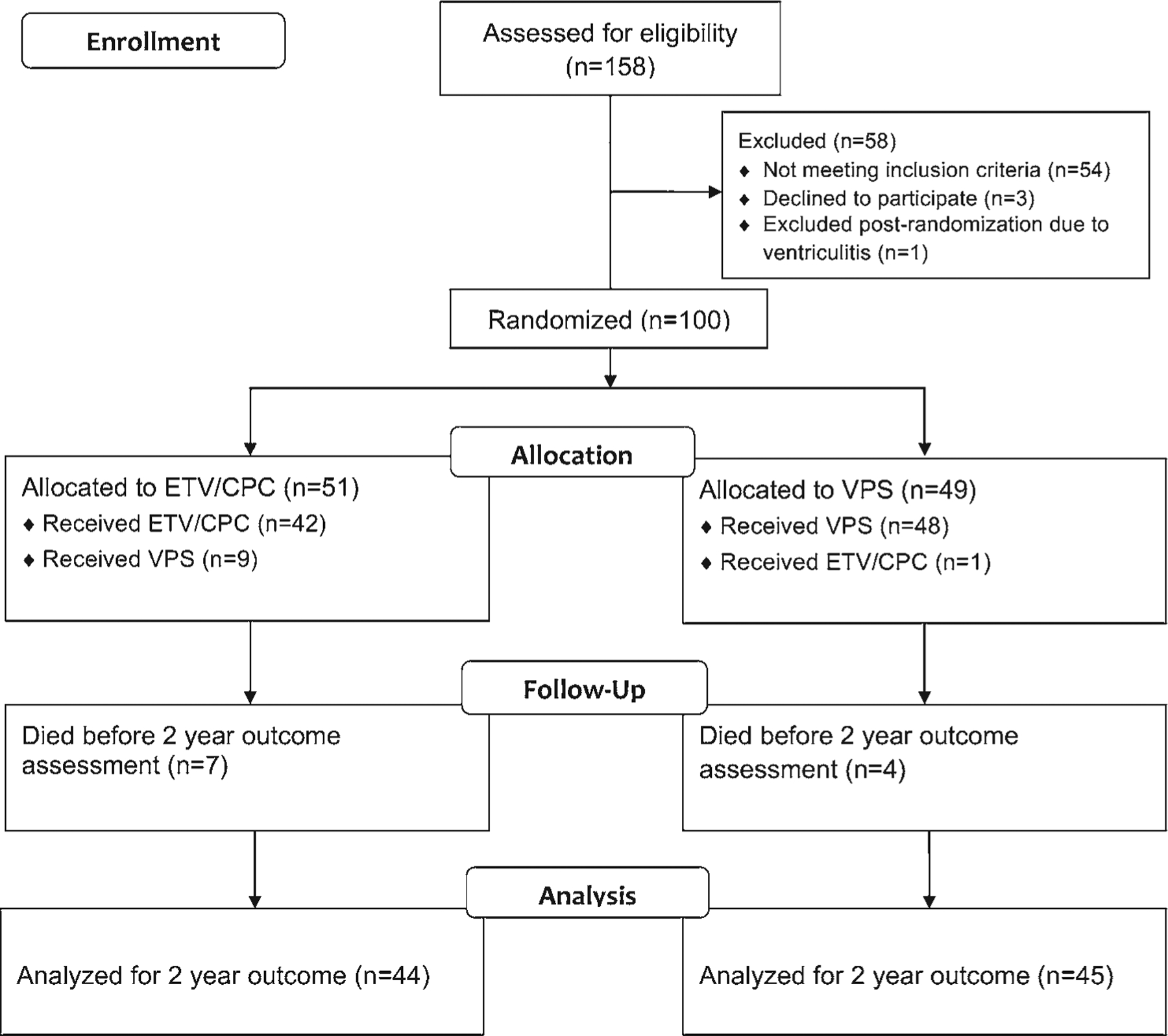
Methods: The authors performed a trial at a single center in Mbale, Uganda, involving infants (age < 180 days old) with postinfectious hydrocephalus randomized to endoscopic third ventriculostomy plus choroid plexus cauterization (ETV+CPC; n = 51) or ventriculoperitoneal shunt (VPS; n = 49). After 2 years, they assessed developmental outcome with the Bayley Scales of Infant Development, Third Edition (BSID-III), and brain volume (raw and normalized for age and sex) with CT scans.
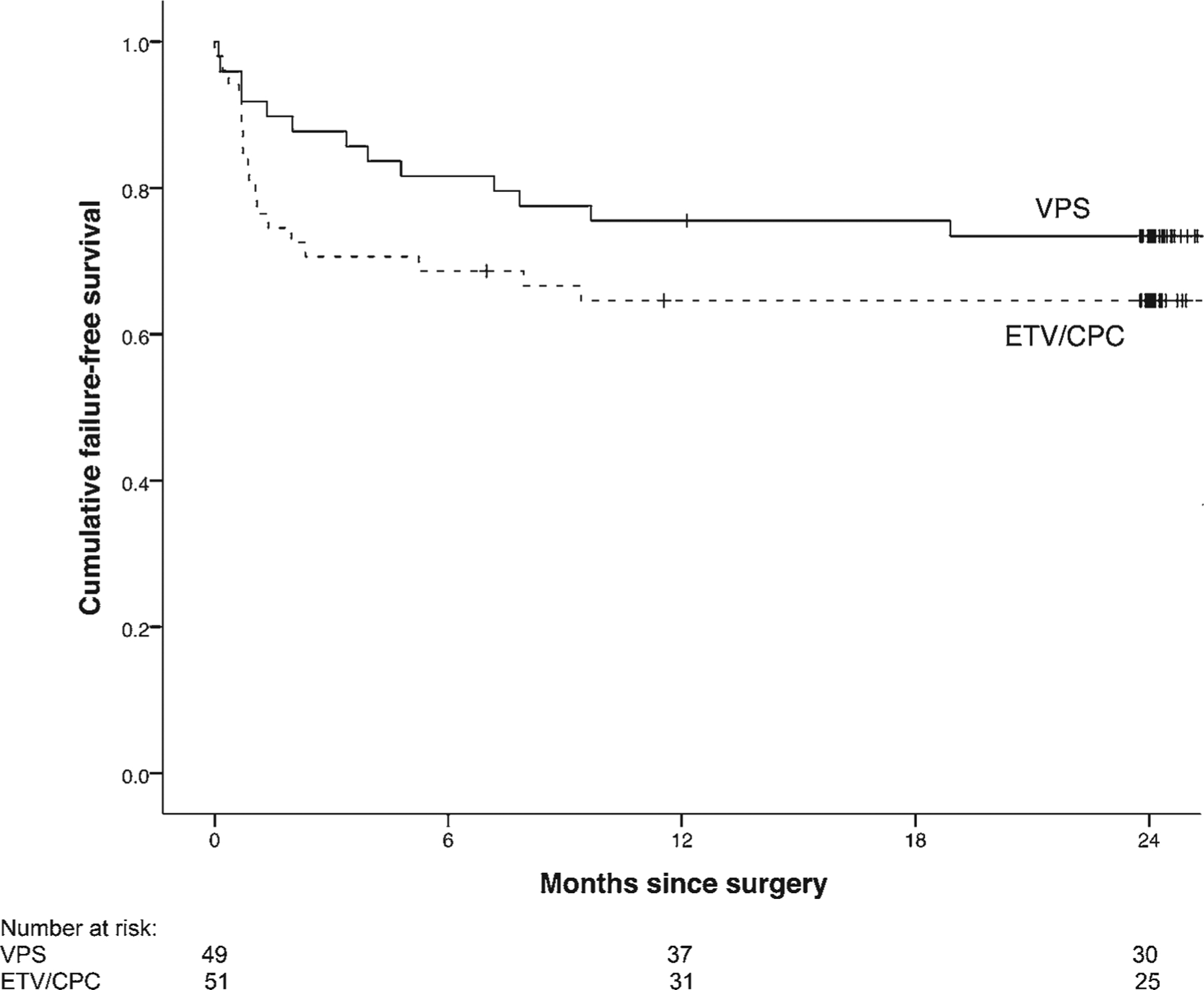
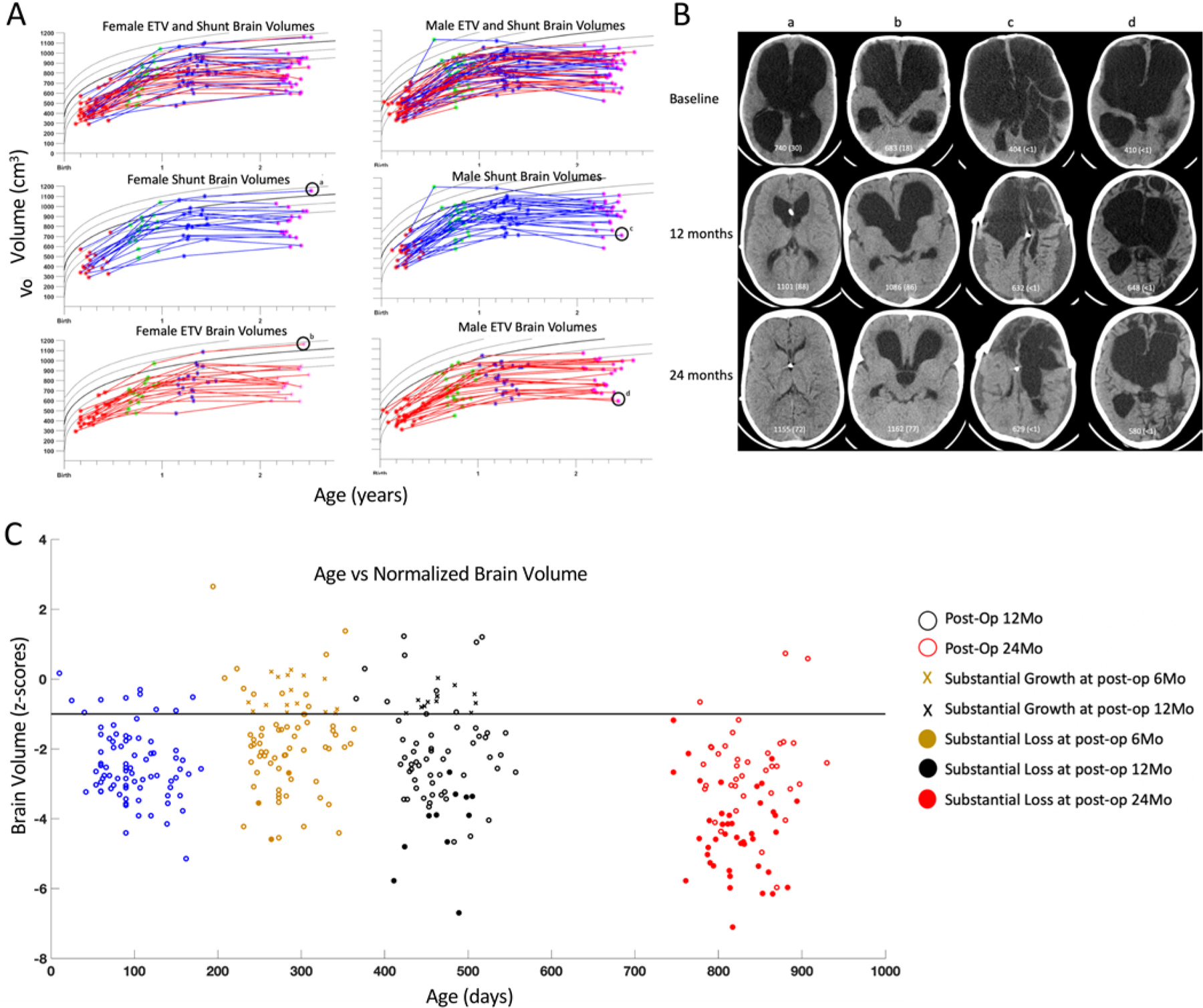
Results: Eighty-nine infants were assessed for 2-year outcome. There were no significant differences between the two surgical treatment arms in terms of BSID-III cognitive score (p = 0.17) or brain volume (p = 0.36), so they were analyzed together. Raw brain volumes increased between baseline and 2 years (p < 0.001), but this increase occurred almost exclusively in the 1st year (p < 0.001). The fraction of patients with a normal brain volume increased from 15.2% at baseline to 50.0% at 1 year but then declined to 17.8% at 2 years. Substantial normalized brain volume loss was seen in 21.3% patients between baseline and year 2 and in 76.7% between years 1 and 2. The extent of brain growth in the 1st year was not associated with the extent of brain volume changes in the 2nd year. There were significant positive correlations between 2-year brain volume and all BSID-III scores and BSID-III changes from baseline.
Conclusions: In Sub-Saharan Africa, even after successful surgical treatment of infant postinfectious hydrocephalus, early posttreatment brain growth stagnates in the 2nd year. While the reasons for this finding are unclear, it further emphasizes the importance of primary infection prevention and mitigation strategies along with optimizing the child's environment to maximize brain growth potential.
Keywords: ETV+CPC; brain growth; choroid plexus cauterization; endoscopic third ventriculostomy; hydrocephalus; neurocognitive outcome; ventriculoperitoneal shunt.
Conflict of interest statement
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Figures
References
-
- Warf BC. Educate one to save a few. Educate a few to save many. World Neurosurg. 2013; 79(2)(suppl): 15.e15–15.e18. - PubMed
-
- Dewan MC, Rattani A, Mekary R, et al. Global hydrocephalus epidemiology and incidence: systematic review and meta-analysis. J Neurosurg. 2018; 130(4): 1–15. - PubMed
-
- Warf BC. Hydrocephalus in Uganda: the predominance of infectious origin and primary management with endoscopic third ventriculostomy. J Neurosurg. 2005; 102(1)(suppl): 1–15. - PubMed
-
- Warf BC, Alkire BC, Bhai S, et al. Costs and benefits of neurosurgical intervention for infant hydrocephalus in sub-Saharan Africa. J Neurosurg Pediatr. 2011; 8(5): 509–521. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
