

Prediagnosis pathway benchmarking audit in patients with Duchenne muscular dystrophy
- PMID: 34244165
- PMCID: PMC8785041
- DOI: 10.1136/archdischild-2020-321451
Prediagnosis pathway benchmarking audit in patients with Duchenne muscular dystrophy
Abstract
Objective: To describe age and time at key stages in the Duchenne muscular dystrophy (DMD) prediagnosis pathway at selected centres to identify opportunities for service improvement.
Design: A multicentre retrospective national audit.
Setting: Nine tertiary neuromuscular centres across the UK and Ireland. A prior single-centre UK audit of 20 patients with no DMD family history provided benchmark criteria.
Patients: Patients with a definitive diagnosis of DMD documented within 3 years prior to December 2018 (n=122).
Main outcome measures: Mean age (months) at four key stages in the DMD diagnostic pathway and mean time (months) of presentational and diagnostic delay, and time from first reported symptoms to definitive diagnosis. Type of symptoms was also recorded.
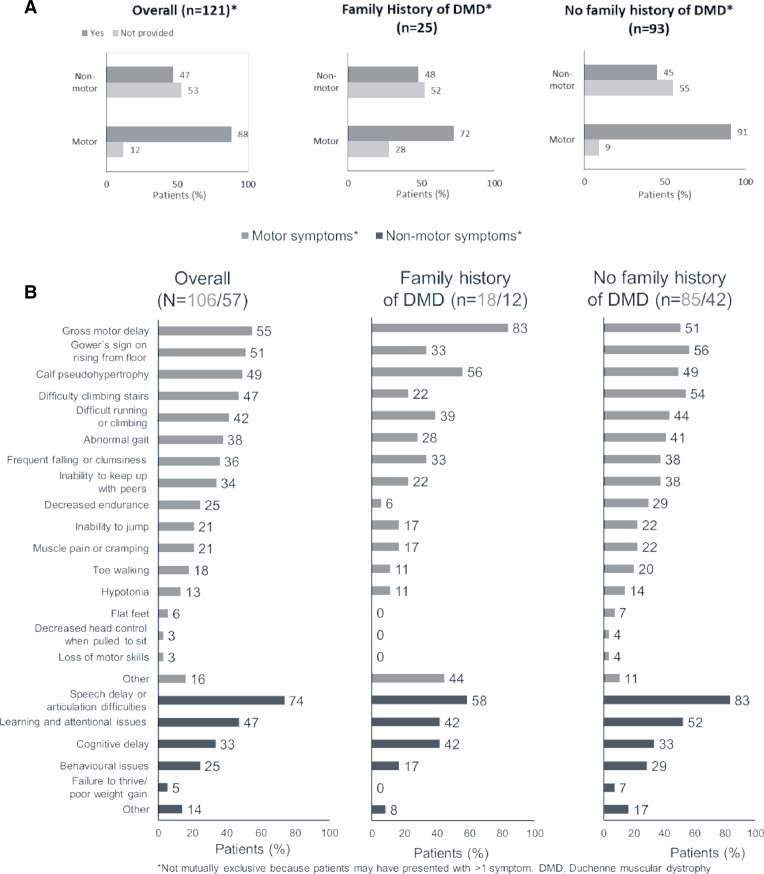
Results: Overall, mean age at definitive diagnosis, age at first engagement with healthcare professional (HCP) and age at first reported symptoms were 53.9±29.7, 49.9±28.9 and 36.4±26.8 months, respectively. The presentational delay and time to diagnosis were 21.1 (±21.1) and 4.6 (±7.9) months, respectively. The mean time from first reported symptoms to definitive diagnosis was 24.2±20.9. The percentages of patients with motor and/or non-motor symptoms recorded were 88% (n=106/121) and 47% (n=57/121), respectively.
Conclusions: Majority of data mirrored the benchmark audit. However, while the time to diagnosis was shorter, a presentational delay was observed. Failure to recognise early symptoms of DMD could be a contributing factor and represents an unmet need in the diagnosis pathway. Methods determining how to improve this need to be explored.
Keywords: audit; epidemiology; neuropathology.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: VLG has received grants from Biogen, PTC Therapeutics, Wave Life Sciences and Catabasis; MF has nothing to disclose; MP has received a grant from PTC Therapeutics; AMC has received fees from PTC Therapeutics in relation to contributions to advisory boards, invited lectures and a presentation; IH has nothing to declare; ST has received conference sponsorship; CGELDG has received grants from PTC Therapeutics; DOR has nothing to declare; DP has nothing to declare; TW has received honorariums for lectures and advisory boards from PTC therapeutics, Biogen, Genzyme Sanofi, Roche, Sarepta and Santhera; SS is an employee of OPEN VIE; ID is employed by PTC Therapeutics.
Figures


References
-
- nhs.uk . Newborn blood spot test [Internet], 2017. Available: https://www.nhs.uk/conditions/pregnancy-and-baby/newborn-blood-spot-test/ [Accessed 06 Jul 2020].
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous