

A pilot study to assess the healing of meniscal tears in young adult goats
- PMID: 34244551
- PMCID: PMC8270994
- DOI: 10.1038/s41598-021-93405-3
A pilot study to assess the healing of meniscal tears in young adult goats
Abstract
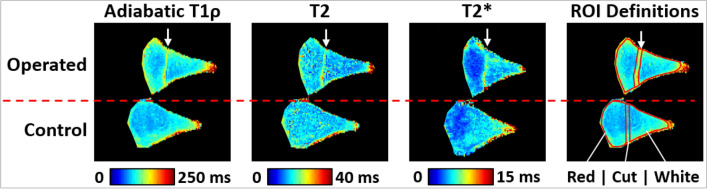
Meniscal tears are a common orthopedic injury, yet their healing is difficult to assess post-operatively. This impedes clinical decisions as the healing status of the meniscus cannot be accurately determined non-invasively. Thus, the objectives of this study were to explore the utility of a goat model and to use quantitative magnetic resonance imaging (MRI) techniques, histology, and biomechanical testing to assess the healing status of surgically induced meniscal tears. Adiabatic T1ρ, T2, and T2* relaxation times were quantified for both operated and control menisci ex vivo. Histology was used to assign healing status, assess compositional elements, and associate healing status with compositional elements. Biomechanical testing determined the failure load of healing lesions. Adiabatic T1ρ, T2, and T2* were able to quantitatively identify different healing states. Histology showed evidence of diminished proteoglycans and increased vascularity in both healed and non-healed menisci with surgically induced tears. Biomechanical results revealed that increased healing (as assessed histologically and on MRI) was associated with greater failure load. Our findings indicate increased healing is associated with greater meniscal strength and decreased signal differences (relative to contralateral controls) on MRI. This indicates that quantitative MRI may be a viable method to assess meniscal tears post-operatively.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures





References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
