

An examination between treatment type and treatment retention in persons with opioid and co-occurring alcohol use disorders
- PMID: 34245997
- PMCID: PMC8370094
- DOI: 10.1016/j.drugalcdep.2021.108886
An examination between treatment type and treatment retention in persons with opioid and co-occurring alcohol use disorders
Abstract
Background and aims: Persons with opioid use disorder (OUD) and co-occurring alcohol use disorder (AUD) are understudied. We identified whether co-occurring AUD was associated with OUD treatment type, compared associations between treatment type and six-month treatment retention and determined whether co-occurring AUD moderated these relationships.
Methods: We used an observational cohort study design to analyze insurance claims data from 2011 to 2016 from persons aged 12-64 with an opioid abuse or opioid dependence diagnosis and OUD treatment claim. Our unit of analysis was the treatment episode; we used logistic regression for analyses.
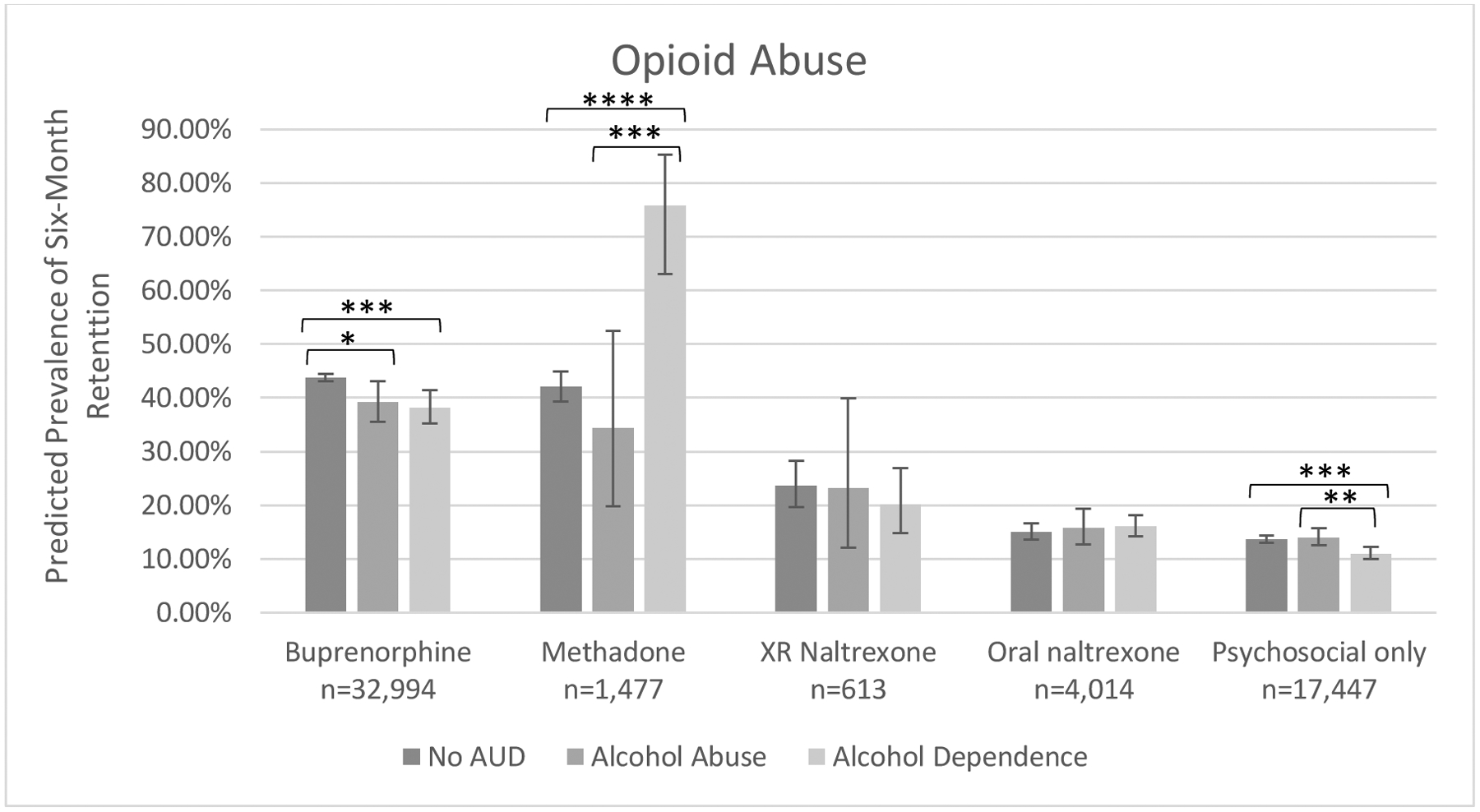
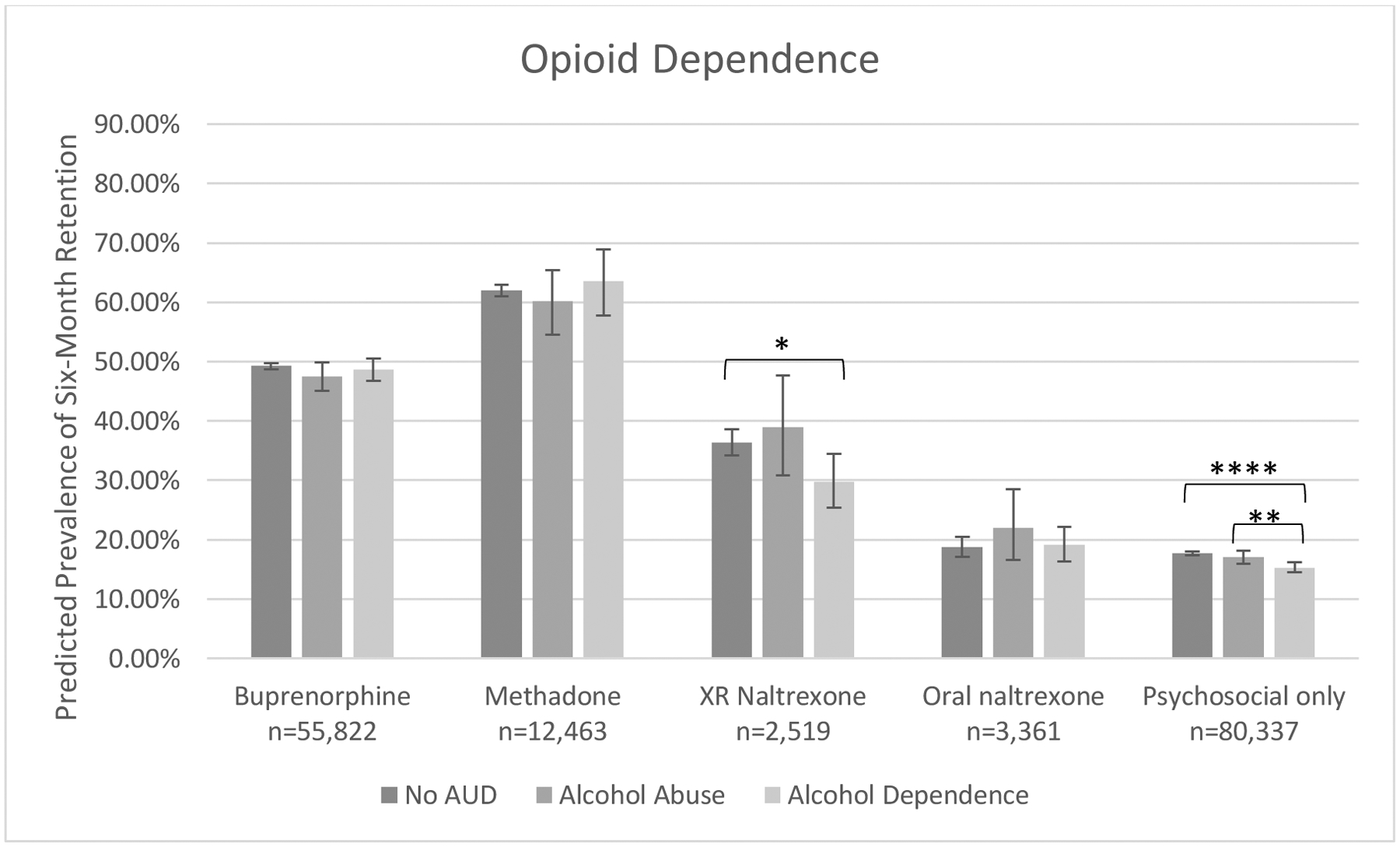
Results: Of 211,047 treatment episodes analyzed, 14 % had co-occurring alcohol abuse or dependence diagnoses. Among persons with opioid dependence, persons with co-occurring alcohol dependence were 25 % less likely to receive medication treatment relative to those without AUD. Further, alcohol dependence was associated with decreased likelihood of treatment with buprenorphine (AOR 0.47, 95 % CI 0.44-0.49) or methadone (AOR 0.31, 95 % CI 0.28-0.35) and increased likelihood of treatment with extended-release (AOR 1.36, 95 % CI 1.21-1.54) or oral (AOR 1.73, 95 % CI 1.57-1.90) naltrexone relative to psychosocial treatment. Buprenorphine and methadone were associated with highest retention prevalence regardless of OUD or AUD severity. Co-occurring alcohol abuse or dependence did not meaningfully change retention prevalence associated with buprenorphine or methadone. Co-occurring AUD was not associated with improved retention among persons receiving either formulation of naltrexone.
Conclusions: Buprenorphine and methadone are associated with relatively high likelihood of treatment retention among persons opioid and alcohol dependence, but are disproportionately under-prescribed.
Keywords: Alcohol use disorder; Buprenorphine; Methadone; Naltrexone; Opioid use disorder; Treatment retention.
Copyright © 2021. Published by Elsevier B.V.
Conflict of interest statement
Conflict of Interest
Dr. Bierut is listed as an inventor on Issued U.S. Patent 8,080,371, “Markers for Addiction” covering the use of certain SNPs in determining the diagnosis, prognosis, and treatment of addiction; Dr. Bierut is a Speaker Bureau member for Imedex. The other authors have indicated they have no potential conflicts of interest to disclose.
Figures
Similar articles
-
Association of Opioid Use Disorder Treatment With Alcohol-Related Acute Events.JAMA Netw Open. 2021 Feb 1;4(2):e210061. doi: 10.1001/jamanetworkopen.2021.0061. JAMA Netw Open. 2021. PMID: 33625511 Free PMC article.
-
Examining differences in retention on medication for opioid use disorder: An analysis of Ohio Medicaid data.J Subst Abuse Treat. 2022 May;136:108686. doi: 10.1016/j.jsat.2021.108686. Epub 2021 Dec 15. J Subst Abuse Treat. 2022. PMID: 34953637
-
Pregnancy Rates Among Women Treated with Medication for Opioid Use Disorder.J Gen Intern Med. 2024 Jun;39(8):1342-1348. doi: 10.1007/s11606-024-08689-8. Epub 2024 Feb 29. J Gen Intern Med. 2024. PMID: 38424347 Free PMC article.
-
Medications for management of opioid use disorder.Am J Health Syst Pharm. 2019 Jul 18;76(15):1097-1103. doi: 10.1093/ajhp/zxz105. Am J Health Syst Pharm. 2019. PMID: 31361869 Review.
-
Medications for Maintenance Treatment of Opioid Use Disorder in Adolescents: A Narrative Review and Assessment of Clinical Benefits and Potential Risks.J Stud Alcohol Drugs. 2019 Jul;80(4):393-402. J Stud Alcohol Drugs. 2019. PMID: 31495374 Review.
Cited by
-
Effects of randomization to buprenorphine or naltrexone for OUD on cannabis use outcomes: A secondary analysis of the X:BOT trial.Drug Alcohol Depend. 2025 Mar 1;268:112550. doi: 10.1016/j.drugalcdep.2025.112550. Epub 2025 Jan 18. Drug Alcohol Depend. 2025. PMID: 39892089 Clinical Trial.
-
Medications for opioid use disorder: Predictors of early discontinuation and reduction of overdose risk in US military veterans by medication type.Addiction. 2025 Jan;120(1):138-151. doi: 10.1111/add.16659. Epub 2024 Sep 7. Addiction. 2025. PMID: 39243190 Free PMC article.
-
Comparative Effectiveness Associated With Buprenorphine and Naltrexone in Opioid Use Disorder and Cooccurring Polysubstance Use.JAMA Netw Open. 2022 May 2;5(5):e2211363. doi: 10.1001/jamanetworkopen.2022.11363. JAMA Netw Open. 2022. PMID: 35536575 Free PMC article.
-
Risks of returning to opioid use at treatment entry and early in opioid use disorder treatment: Role of non-opioid substances.Drug Alcohol Depend. 2023 Oct 1;251:110926. doi: 10.1016/j.drugalcdep.2023.110926. Epub 2023 Aug 9. Drug Alcohol Depend. 2023. PMID: 37604012 Free PMC article.
-
Gabapentin increases the abuse liability of alcohol alone and in combination with oxycodone in participants with co-occurring opioid and alcohol use disorder.Pharmacol Biochem Behav. 2022 Nov;221:173482. doi: 10.1016/j.pbb.2022.173482. Epub 2022 Oct 13. Pharmacol Biochem Behav. 2022. PMID: 36244527 Free PMC article. Clinical Trial.
References
-
- Anton RF, O’Malley SS, Ciraulo DA, Cisler RA, Couper D, Donovan DM, Gastfriend DR, Hosking JD, Johnson BA, LoCastro JS, Longabaugh R, Mason BJ, Mattson ME, Miller WR, Pettinati HM, Randall CL, Swift R, Weiss RD, Williams LD, Zweben A, Group CSR, 2006. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA 295(17), 2003–2017. - PubMed
-
- Bogdanowicz KM, Stewart R, Broadbent M, Hatch SL, Hotopf M, Strang J, Hayes RD, 2015. Double trouble: Psychiatric comorbidity and opioid addiction-all-cause and cause-specific mortality. Drug Alcohol Depend 148, 85–92. - PubMed
-
- Darke S, Zador D, 1996. Fatal heroin ‘overdose’: a review. Addiction 91(12), 1765–1772. - PubMed
-
- Dole VP, Nyswander M, 1965. A Medical Treatment for Diacetylmorphine (Heroin) Addiction. A Clinical Trial with Methadone Hydrochloride. JAMA 193, 646–650. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
