

Rehabilitation Intervention in Older Patients With Acute Heart Failure With Preserved Versus Reduced Ejection Fraction
- PMID: 34246602
- PMCID: PMC8487922
- DOI: 10.1016/j.jchf.2021.05.007
Rehabilitation Intervention in Older Patients With Acute Heart Failure With Preserved Versus Reduced Ejection Fraction
Abstract
Objectives: This study assessed for treatment interactions by ejection fraction (EF) subgroup (≥45% [heart failure with preserved ejection fraction (HFpEF); vs <45% [heart failure with reduced ejection fraction (HFrEF)]).
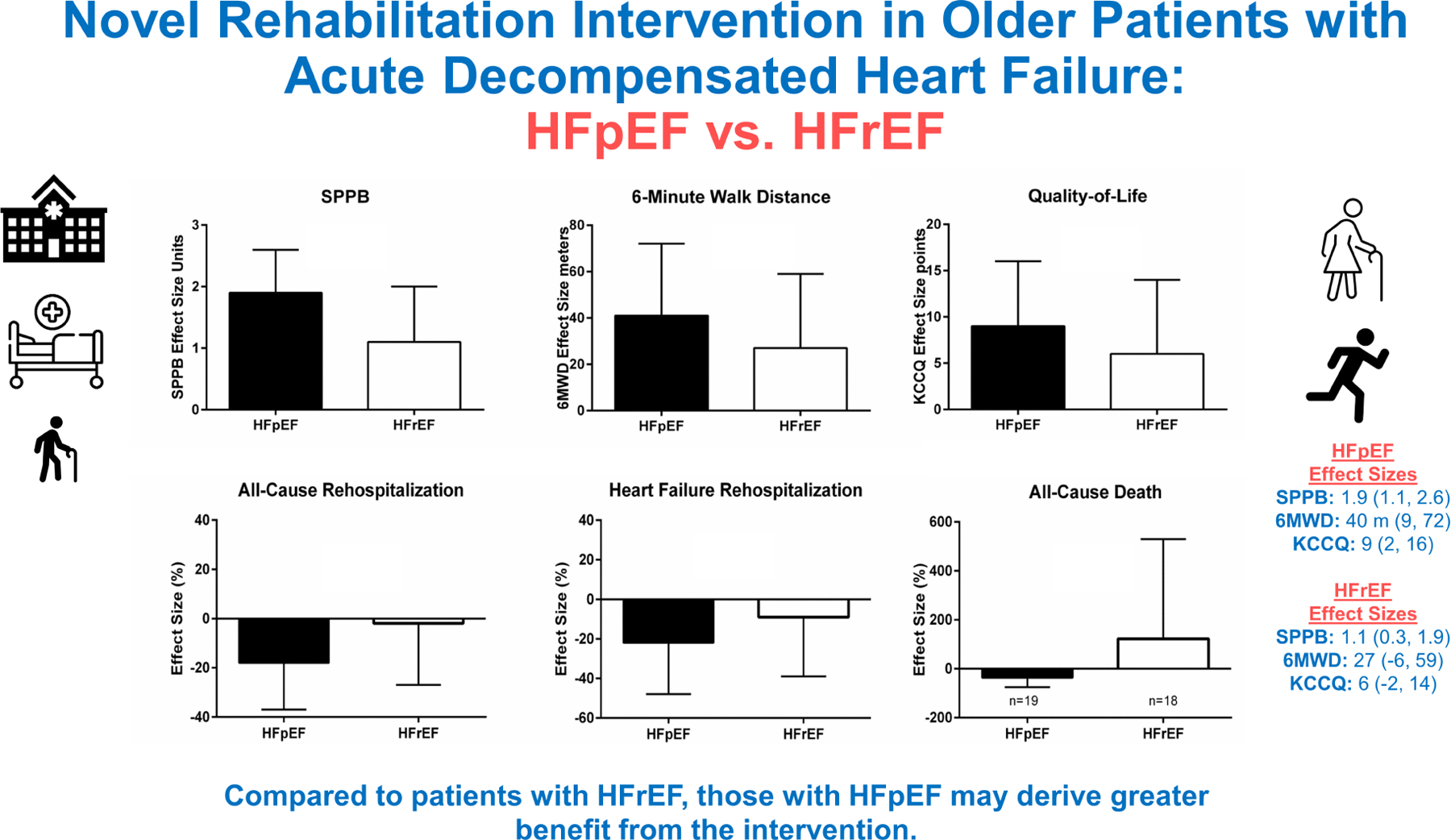
Background: The REHAB-HF trial showed that an early multidomain rehabilitation intervention improved physical function, frailty, quality-of-life, and depression in older patients hospitalized with acute decompensated heart failure (ADHF).
Methods: Three-month outcomes were: Short Physical Performance Battery (SPPB), 6-min walk distance (6MWD), and Kansas City Cardiomyopathy Questionnaire (KCCQ). Six-month end points included all-cause rehospitalization and death and a global rank of death, all-cause rehospitalization, and SPPB. Prespecified significance level for interaction was P ≤ 0.1.
Results: Among 349 total participants, 185 (53%) had HFpEF and 164 (47%) had HFrEF. Compared with HFrEF, HFpEF participants were more often women (61% vs 43%) and had significantly worse baseline physical function, frailty, quality of life, and depression. Although interaction P values for 3-month outcomes were not significant, effect sizes were larger for HFpEF vs HFrEF: SPPB +1.9 (95% CI: 1.1-2.6) vs +1.1 (95% CI: 0.3-1.9); 6MWD +40 meters (95% CI: 9 meters-72 meters) vs +27 (95% CI: -6 meters to 59 meters); KCCQ +9 (2-16) vs +6 (-2 to 14). All-cause rehospitalization rate was nominally lower with intervention in HFpEF but not HFrEF [effect size 0.83 (95% CI: 0.64-1.09) vs 0.99 (95% CI: 0.74-1.33); interaction P = 0.40]. There were significantly greater treatment benefits in HFpEF vs HFrEF for all-cause death [interaction P = 0.08; intervention rate ratio 0.63 (95% CI: 0.25-1.61) vs 2.21 (95% CI: 0.78-6.25)], and the global rank end point (interaction P = 0.098) with benefit seen in HFpEF [probability index 0.59 (95% CI: 0.50-0.68)] but not HFrEF.
Conclusions: Among older patients hospitalized with ADHF, compared with HFrEF those with HFpEF had significantly worse impairments at baseline and may derive greater benefit from the intervention. (A Trial of Rehabilitation Therapy in Older Acute Heart Failure Patients [REHAB-HF]; NCT02196038).
Keywords: HFpEF; aging; heart failure; physical function; rehabilitation.
Copyright © 2021 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures This study was supported in part by the National Institutes of Health (research grants R01AG045551, R01AG18915, P30AG021332, P30AG028716, and U24AG059624). Support was also provided in part by the Kermit Glenn Phillips II Chair in Cardiovascular Medicine and the Oristano Family Fund at Wake Forest School of Medicine. Dr Mentz received research support and honoraria from Abbott, American Regent, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Cytokinetics, Medtronic, Merck, Novartis, Roche, Sanofi, and Vifor. Dr Whellan received research support and consulting fees from Amgen, CVRx, Cytokinetics, Fibrogen, Novartis, and NovoNordisk. Dr Upadhya received research support from Novartis and Corvia. Dr Reed received research support from Abbott, AstraZeneca, Janssen Research and Development, Lundbeck, Monteris, and Merck; and received consulting with Minomic International, SVC Systems, and Regeneron Pharmaceuticals. Dr Kitzman received honoraria outside the present study as a consultant for Bayer, Merck, Medtronic, Relypsa, Merck, Corvia Medical, Boehringer-Ingelheim, NovoNordisk, AstraZeneca, and Novartis; grant funding outside the present study from Novartis, Bayer, NovoNordisk, and AstraZeneca; and has stock ownership in Gilead Sciences. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Shah KS, Xu H, Matsouaka RA et al. Heart Failure With Preserved, Borderline, and Reduced Ejection Fraction: 5-Year Outcomes. Journal of the American College of Cardiology 2017;70:2476–2486. - PubMed
-
- Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM. Trends in prevalence and outcome of heart failure with preserved ejection fraction. The New England Journal of Medicine 2006;355:251–9. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
