

Quantifying and Understanding the Higher Risk of Atherosclerotic Cardiovascular Disease Among South Asian Individuals: Results From the UK Biobank Prospective Cohort Study
- PMID: 34247495
- PMCID: PMC8355171
- DOI: 10.1161/CIRCULATIONAHA.120.052430
Quantifying and Understanding the Higher Risk of Atherosclerotic Cardiovascular Disease Among South Asian Individuals: Results From the UK Biobank Prospective Cohort Study
Abstract
Background: Individuals of South Asian ancestry represent 23% of the global population, corresponding to 1.8 billion people, and have substantially higher risk of atherosclerotic cardiovascular disease compared with most other ethnicities. US practice guidelines now recognize South Asian ancestry as an important risk-enhancing factor. The magnitude of enhanced risk within the context of contemporary clinical care, the extent to which it is captured by existing risk estimators, and its potential mechanisms warrant additional study.
Methods: Within the UK Biobank prospective cohort study, 8124 middle-aged participants of South Asian ancestry and 449 349 participants of European ancestry who were free of atherosclerotic cardiovascular disease at the time of enrollment were examined. The relationship of ancestry to risk of incident atherosclerotic cardiovascular disease-defined as myocardial infarction, coronary revascularization, or ischemic stroke-was assessed with Cox proportional hazards regression, along with examination of a broad range of clinical, anthropometric, and lifestyle mediators.
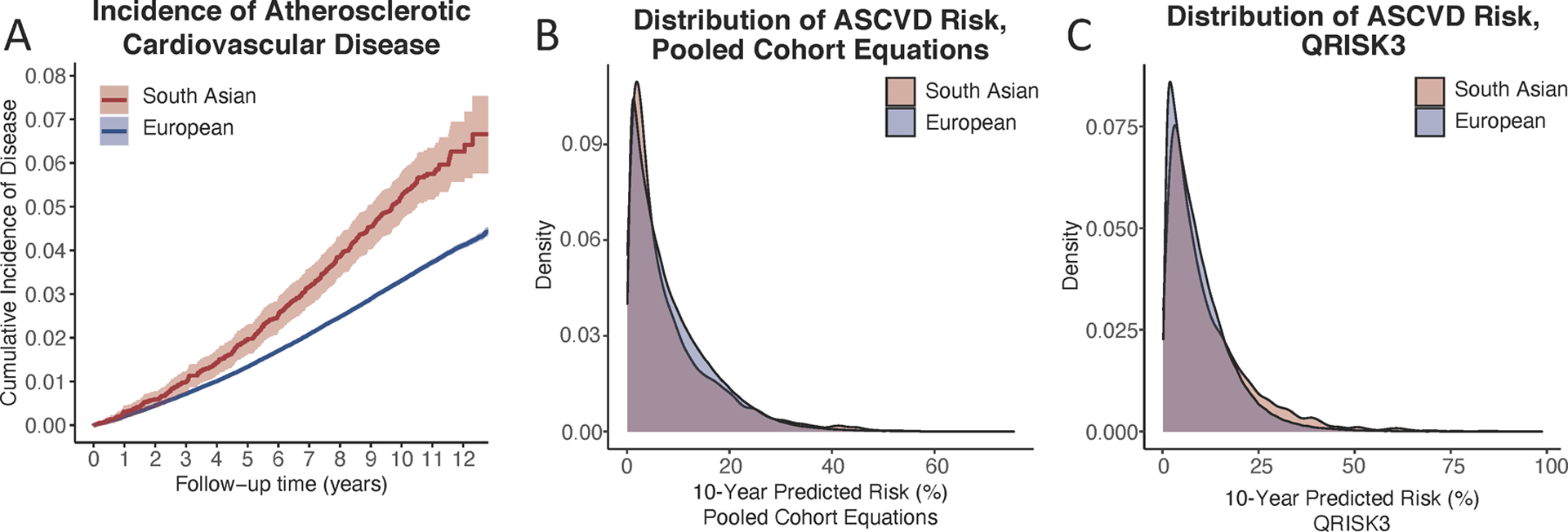
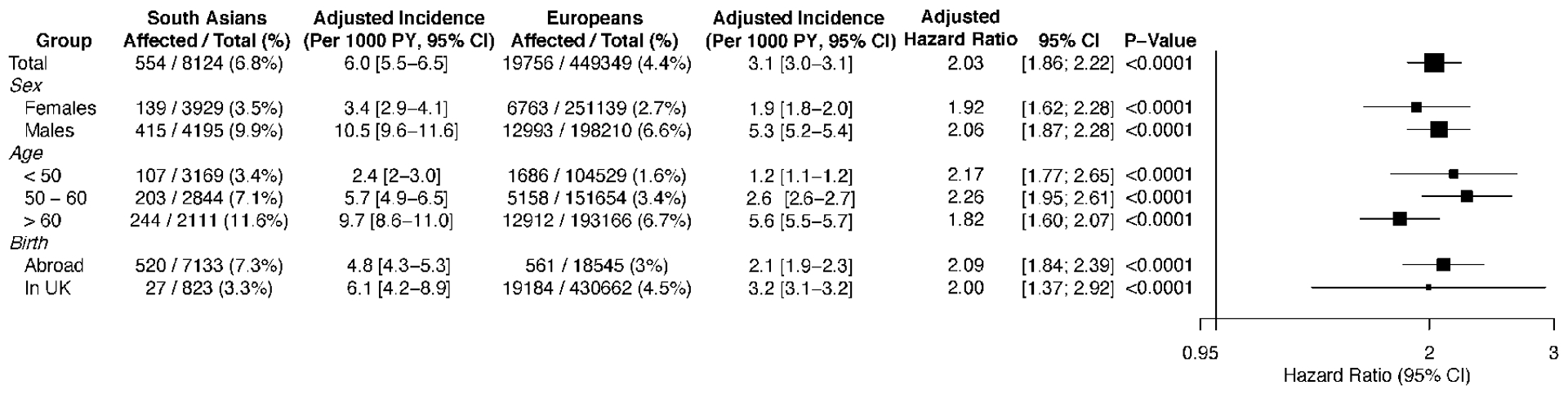
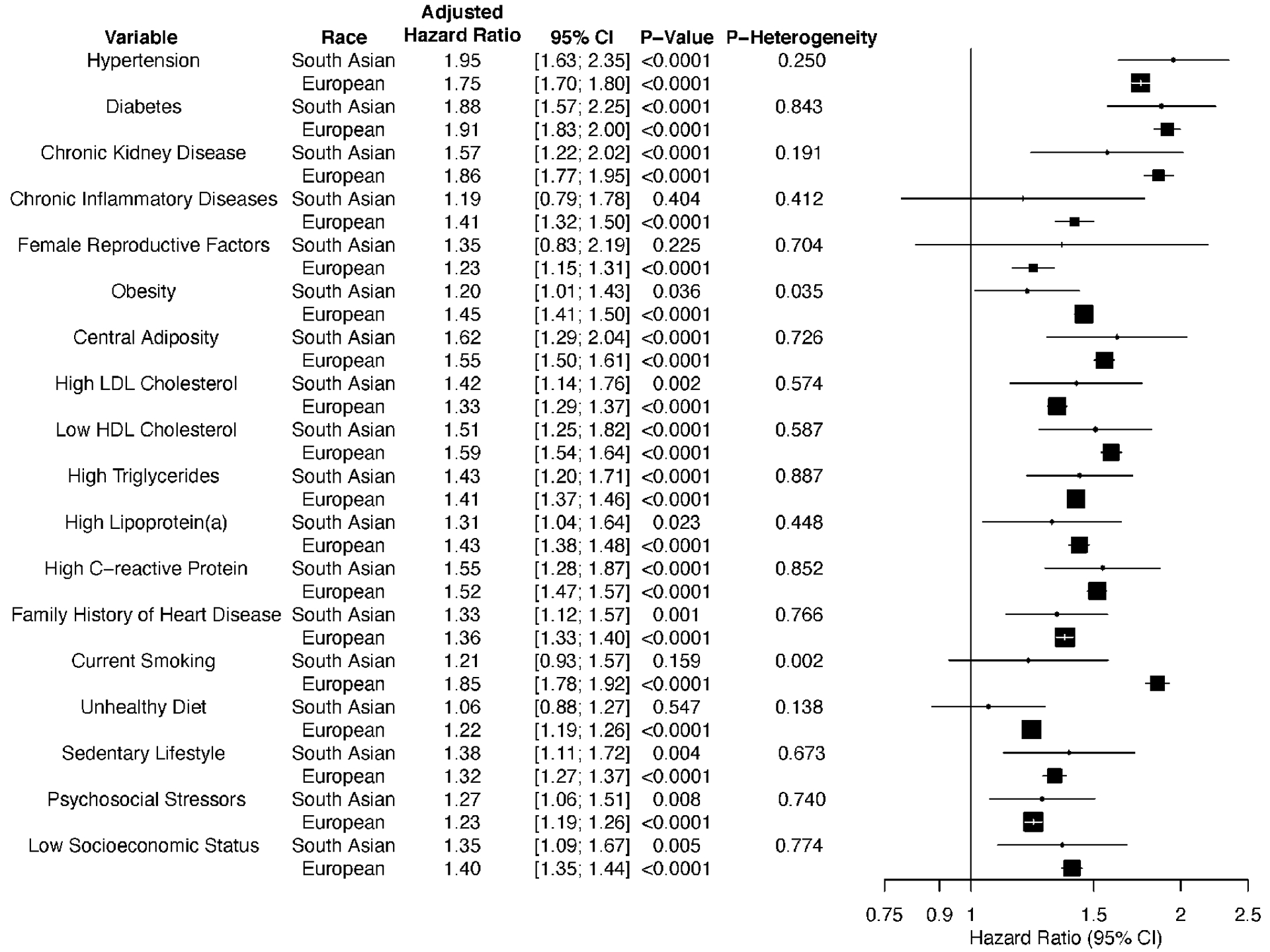
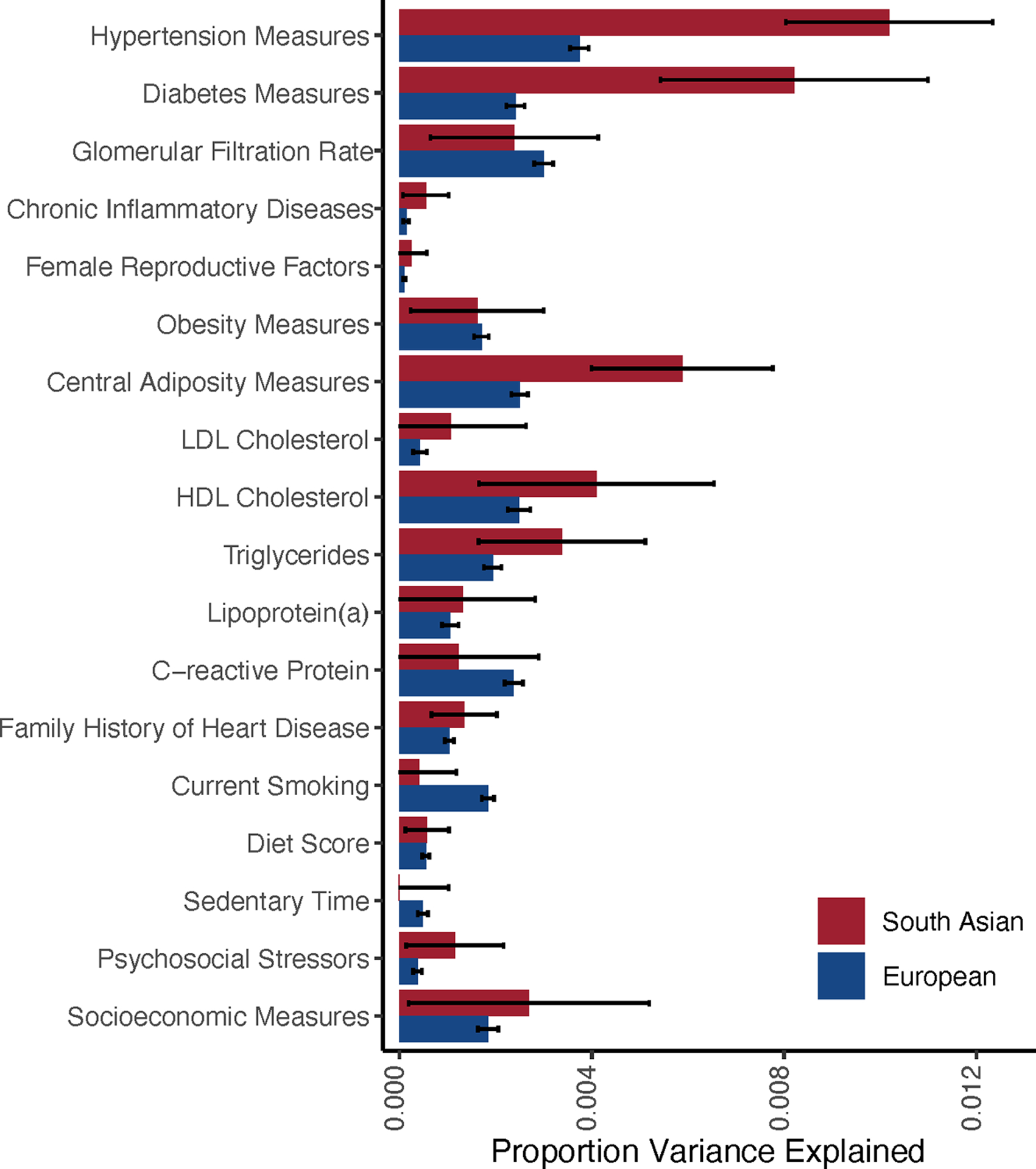
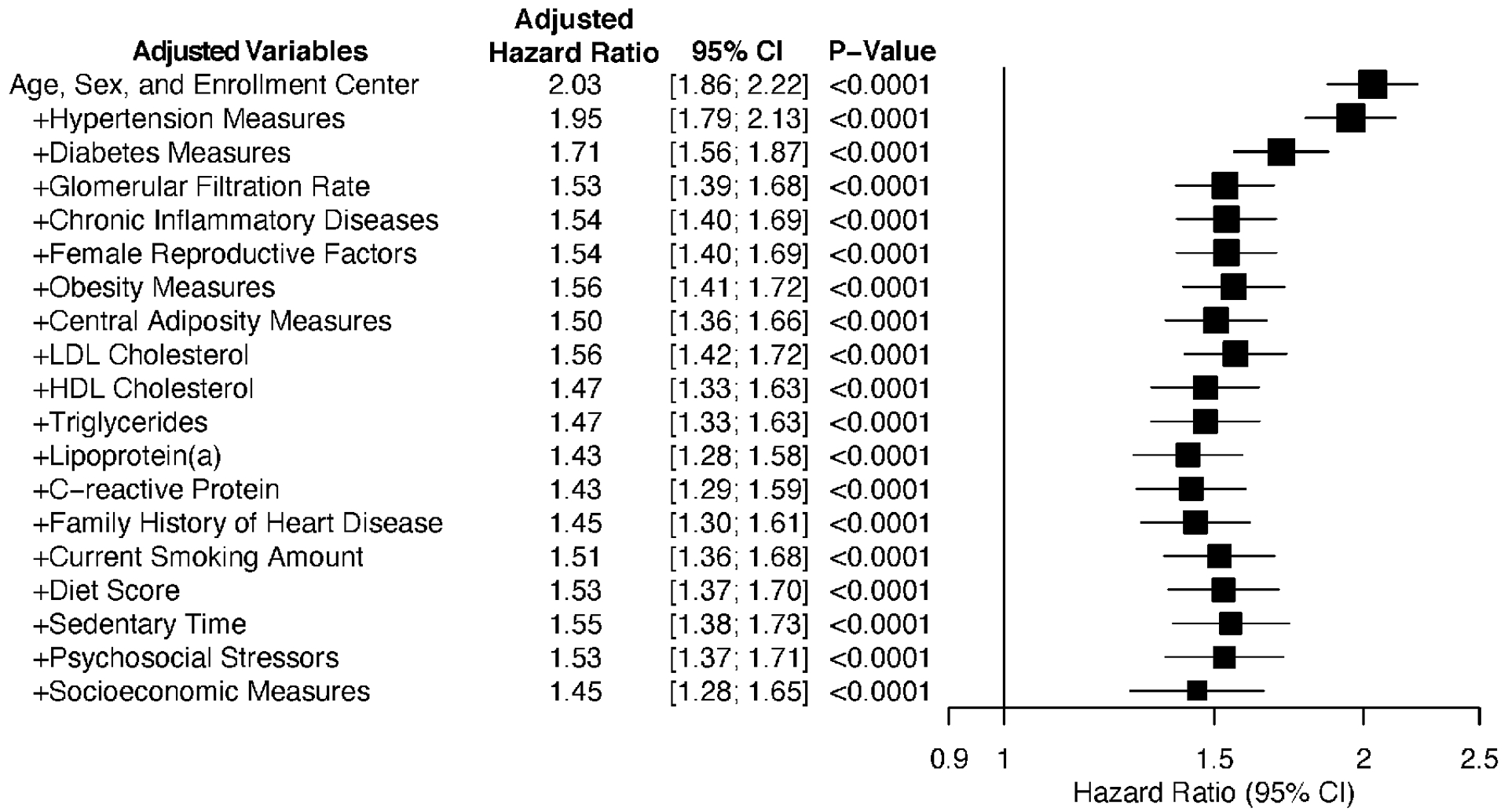
Results: The mean age at study enrollment was 57 years, and 202 405 (44%) were male. Over a median follow-up of 11 years, 554 of 8124 (6.8%) individuals of South Asian ancestry experienced an atherosclerotic cardiovascular disease event compared with 19 756 of 449 349 (4.4%) individuals of European ancestry, corresponding to an adjusted hazard ratio of 2.03 (95% CI, 1.86-2.22; P<0.001). This higher relative risk was largely consistent across a range of age, sex, and clinical subgroups. Despite the >2-fold higher observed risk, the predicted 10-year risk of cardiovascular disease according to the American Heart Association/American College of Cardiology Pooled Cohort equations and QRISK3 equations was nearly identical for individuals of South Asian and European ancestry. Adjustment for a broad range of clinical, anthropometric, and lifestyle risk factors led to only modest attenuation of the observed hazard ratio to 1.45 (95% CI, 1.28-1.65, P<0.001). Assessment of variance explained by 18 candidate risk factors suggested greater importance of hypertension, diabetes, and central adiposity in South Asian individuals.
Conclusions: Within a large prospective study, South Asian individuals had substantially higher risk of atherosclerotic cardiovascular disease compared with individuals of European ancestry, and this risk was not captured by the Pooled Cohort Equations.
Keywords: continental population groups; ethnic groups; ischemic stroke; myocardial infarction; risk; risk factor.
Conflict of interest statement
DISCLOSURES:
U.K. and K.N. are employees of IBM Research. A.V.K. has served as a scientific advisor to Sanofi, Medicines Company, Maze Pharmaceuticals, Navitor Pharmaceuticals, Verve Therapeutics, Amgen, Color, and Columbia University (NIH); received speaking fees from Illumina, MedGenome, Amgen, and the Novartis Institute for Biomedical Research and received sponsored research agreements from the Novartis Institute for Biomedical Research and IBM Research. The remaining authors have no disclosures.
Figures


Comment in
-
The South Asian Enigma: Solving a Puzzle of Global Importance.Circulation. 2021 Aug 10;144(6):423-425. doi: 10.1161/CIRCULATIONAHA.121.055159. Epub 2021 Jul 12. Circulation. 2021. PMID: 34247493 Free PMC article. No abstract available.
-
Response by Patel and Khera to Letter Regarding Article, "Quantifying and Understanding the Higher Risk of Atherosclerotic Cardiovascular Disease Among South Asian Individuals: Results From the UK Biobank Prospective Cohort Study".Circulation. 2022 Feb;145(5):e147-e148. doi: 10.1161/CIRCULATIONAHA.121.058059. Epub 2022 Jan 31. Circulation. 2022. PMID: 35100017 Free PMC article. No abstract available.
-
Letter by Enas and Varkey Regarding Article, "Quantifying and Understanding the Higher Risk of Atherosclerotic Cardiovascular Disease Among South Asian Individuals: Results From the UK Biobank Prospective Cohort Study".Circulation. 2022 Feb;145(5):e146. doi: 10.1161/CIRCULATIONAHA.121.056750. Epub 2022 Jan 31. Circulation. 2022. PMID: 35100018 No abstract available.
References
-
- Heron M CDC stacks. Deaths: leading causes for 2017 – 79488. Stephen B. Thacker CDC Library collection Accessed2019 Sep 22. Available from: https://stacks.cdc.gov/view/cdc/79488.
-
- World Health Organization. The top 10 causes of death. December 9, 2020 Accessed2020 Jun 13. Available from: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
-
- Central Intelligence Agency. South Asia: India — The World Factbook - Central Intelligence Agency. Accessed2020 Jul 30. Available from: https://www.cia.gov/library/publications/the-world-factbook/geos/in.html.
-
- US Census Bureau UCBPI. 2010 Census Shows Asians are Fastest-Growing Race Group. Accessed2020 Sep 9. Available from: https://www.census.gov/newsroom/releases/archives/2010_census/cb12-cn22.....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
