

Inflammation and tumor progression: signaling pathways and targeted intervention
- PMID: 34248142
- PMCID: PMC8273155
- DOI: 10.1038/s41392-021-00658-5
Inflammation and tumor progression: signaling pathways and targeted intervention
Abstract
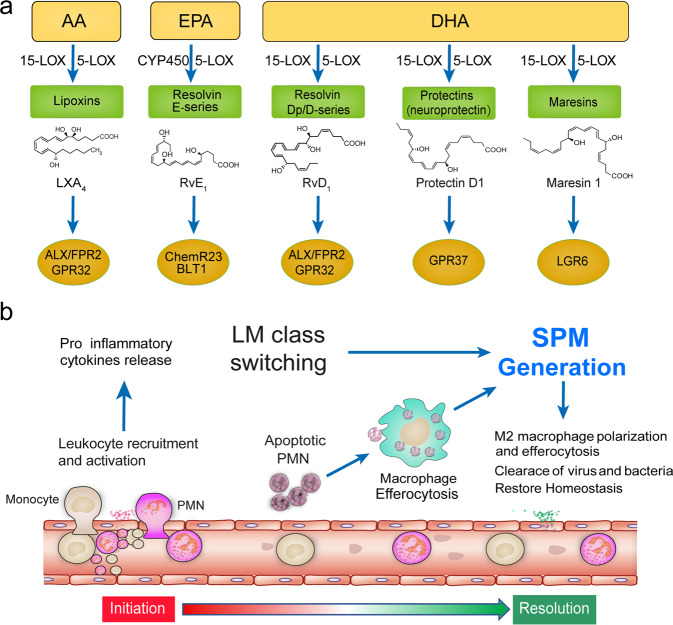
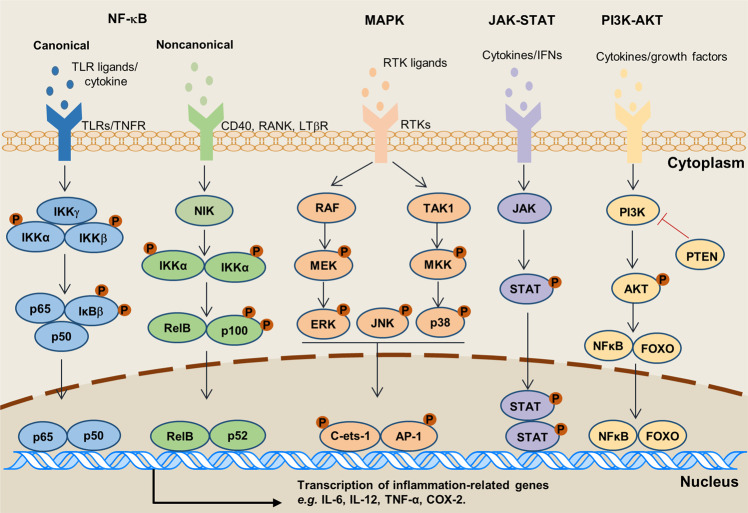
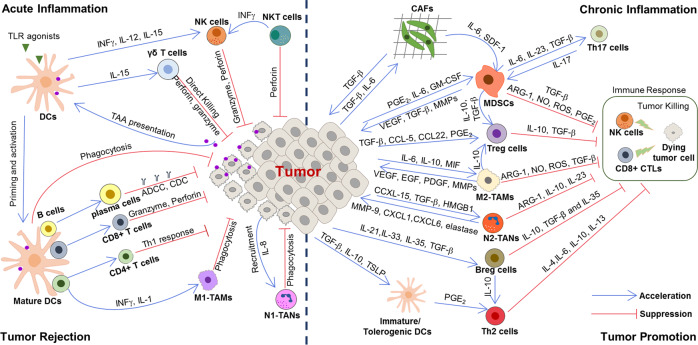
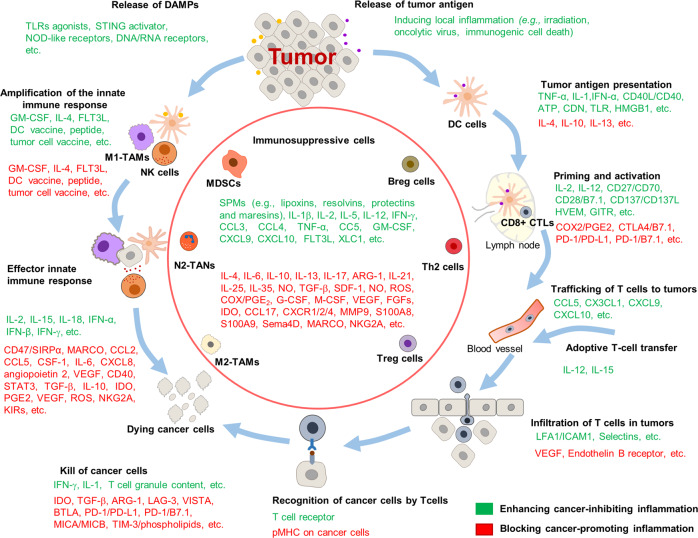
Cancer development and its response to therapy are regulated by inflammation, which either promotes or suppresses tumor progression, potentially displaying opposing effects on therapeutic outcomes. Chronic inflammation facilitates tumor progression and treatment resistance, whereas induction of acute inflammatory reactions often stimulates the maturation of dendritic cells (DCs) and antigen presentation, leading to anti-tumor immune responses. In addition, multiple signaling pathways, such as nuclear factor kappa B (NF-kB), Janus kinase/signal transducers and activators of transcription (JAK-STAT), toll-like receptor (TLR) pathways, cGAS/STING, and mitogen-activated protein kinase (MAPK); inflammatory factors, including cytokines (e.g., interleukin (IL), interferon (IFN), and tumor necrosis factor (TNF)-α), chemokines (e.g., C-C motif chemokine ligands (CCLs) and C-X-C motif chemokine ligands (CXCLs)), growth factors (e.g., vascular endothelial growth factor (VEGF), transforming growth factor (TGF)-β), and inflammasome; as well as inflammatory metabolites including prostaglandins, leukotrienes, thromboxane, and specialized proresolving mediators (SPM), have been identified as pivotal regulators of the initiation and resolution of inflammation. Nowadays, local irradiation, recombinant cytokines, neutralizing antibodies, small-molecule inhibitors, DC vaccines, oncolytic viruses, TLR agonists, and SPM have been developed to specifically modulate inflammation in cancer therapy, with some of these factors already undergoing clinical trials. Herein, we discuss the initiation and resolution of inflammation, the crosstalk between tumor development and inflammatory processes. We also highlight potential targets for harnessing inflammation in the treatment of cancer.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
