

Treatment of Traumatic Intracranial Pseudoaneurysms: A Single-Center Experience
- PMID: 34248827
- PMCID: PMC8267006
- DOI: 10.3389/fneur.2021.690284
Treatment of Traumatic Intracranial Pseudoaneurysms: A Single-Center Experience
Abstract
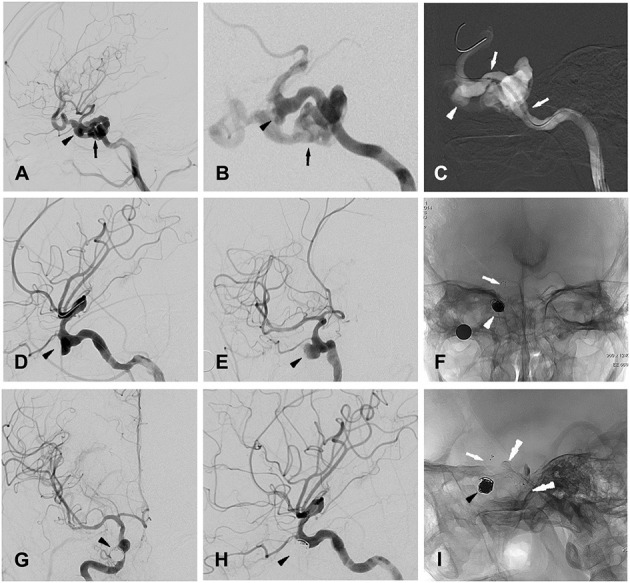
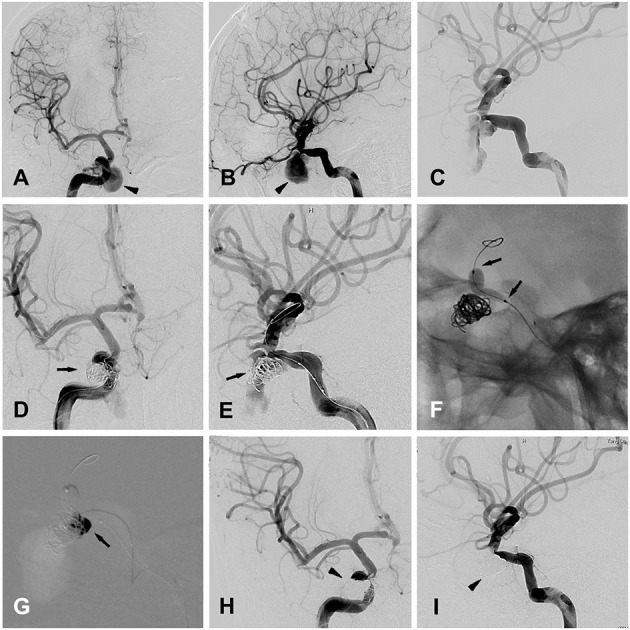
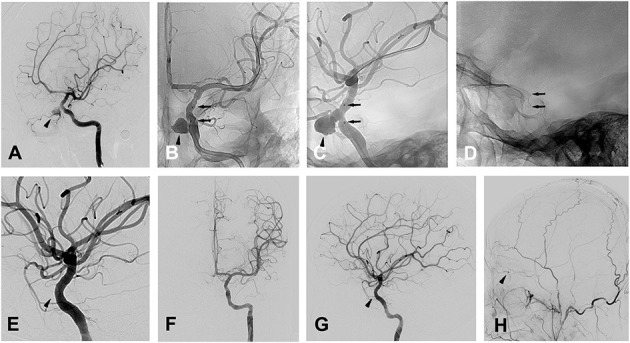
Background and Purpose: As a rare lesion secondary to brain trauma, traumatic intracranial aneurysms (TICAs) lead to high mortality and morbidity, and multiple treatment modalities have been applied for TICAs. All patients diagnosed with TICAs in our institution from 2010 to 2020 were included in the report, and their clinical features, treatment, and outcomes are described in detail. The purpose of this study is to illustrate the characteristic of different therapeutic methods of TICAs, and focus on the endovascular treatment. Methods: A total of 20 patients were included in this study. The 3 patients who declined treatment all died. Five of the other 17 patients were treated surgically, including clipping, wrapping, and trapping with or without EC-IC high-flow bypass, with only 1 case of parent artery preservation. Twelve patients underwent endovascular treatment, including bare coil embolization (1 case), stent-assisted coiling (2 cases), balloon-assisted coils/Onyx glue embolization (1 case) and covered stents (8 cases), with only 1 case of parent artery sacrifice. Results: 20 patients were included in the present study with 17 males, and the mean of age on 27 years (IQR: 22, 44 years). Eight patients presented with epistaxis, followed by 5 patients with coma, 3 patients with visual defects and 2 patients with CSF leakage. There were 18 TICAs located at the internal carotid artery (ICA); The other 2 TICAs located at pericallosal artery and A1 segment anterior cerebral artery (ACA). One case of diplopia occurred due to sacrifice of the ICA. Occlusion of the ophthalmic artery occurred in 3 patients after placement of a covered stent, with 1 patient suffering an irreversible vision decrease. None of the other patients who underwent the treatment have experienced an aggravation of their symptoms since the treatment; During the imaging follow-up, 1 case of recurrence and 1 case of endoleak occurred in this case series. Conclusions: TICAs are associated with significant morbidity and mortality, and endovascular treatment has emerged as a valuable option, which may be promising to improve the clinical outcomes due to their advantages of preserving the parent artery if occlusion of the side branch artery can be avoided.
Keywords: endovascular treatment; parent artery; side branch artery; surgical treatment; traumatic intracranial pseudoaneurysms.
Copyright © 2021 Shi, Gao, Liu, Cui, Zhou, Wang, Yu, Zhang, Qu, Deng and Ge.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous