

Optimising Treatment Outcomes for Children and Adults Through Rapid Genome Sequencing of Sepsis Pathogens. A Study Protocol for a Prospective, Multi-Centre Trial (DIRECT)
- PMID: 34249774
- PMCID: PMC8261237
- DOI: 10.3389/fcimb.2021.667680
Optimising Treatment Outcomes for Children and Adults Through Rapid Genome Sequencing of Sepsis Pathogens. A Study Protocol for a Prospective, Multi-Centre Trial (DIRECT)
Abstract
Background: Sepsis contributes significantly to morbidity and mortality globally. In Australia, 20,000 develop sepsis every year, resulting in 5,000 deaths, and more than AUD$846 million in expenditure. Prompt, appropriate antibiotic therapy is effective in improving outcomes in sepsis. Conventional culture-based methods to identify appropriate therapy have limited yield and take days to complete. Recently, nanopore technology has enabled rapid sequencing with real-time analysis of pathogen DNA. We set out to demonstrate the feasibility and diagnostic accuracy of pathogen sequencing direct from clinical samples, and estimate the impact of this approach on time to effective therapy when integrated with personalised software-guided antimicrobial dosing in children and adults on ICU with sepsis.
Methods: The DIRECT study is a pilot prospective, non-randomized multicentre trial of an integrated diagnostic and therapeutic algorithm combining rapid direct pathogen sequencing and software-guided, personalised antibiotic dosing in children and adults with sepsis on ICU.
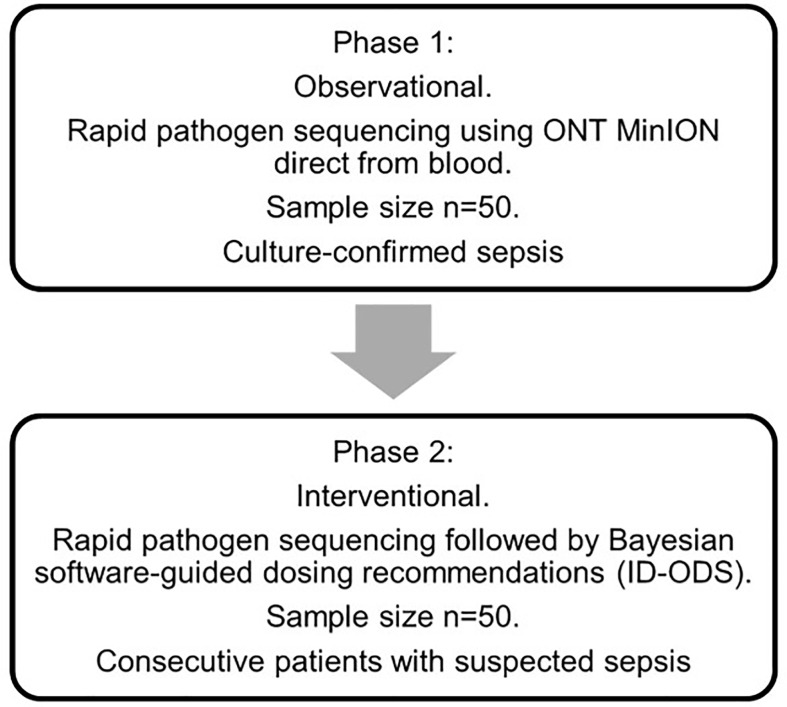
Participants and interventions: DIRECT will collect microbiological and pharmacokinetic samples from approximately 200 children and adults with sepsis admitted to one of four ICUs in Brisbane. In Phase 1, we will evaluate Oxford Nanopore Technologies MinION sequencing direct from blood in 50 blood culture-proven sepsis patients recruited from consecutive patients with suspected sepsis. In Phase 2, a further 50 consecutive patients with suspected sepsis will be recruited in whom MinION sequencing will be combined with Bayesian software-guided (ID-ODS) personalised antimicrobial dosing.
Outcome measures: The primary outcome is time to effective antimicrobial therapy, defined as trough drug concentrations above the MIC of the pathogen. Secondary outcomes are diagnostic accuracy of MinION sequencing from whole blood, time to pathogen identification and susceptibility testing using sequencing direct from whole blood and from positive blood culture broth.
Discussion: Rapid pathogen sequencing coupled with antimicrobial dosing software has great potential to overcome the limitations of conventional diagnostics which often result in prolonged inappropriate antimicrobial therapy. Reduced time to optimal antimicrobial therapy may reduce sepsis mortality and ICU length of stay. This pilot study will yield key feasibility data to inform further, urgently needed sepsis studies. Phase 2 of the trial protocol is registered with the ANZCTR (ACTRN12620001122943).
Trial registration: Registered with the Australia New Zealand Clinical Trials Registry Number ACTRN12620001122943.
Keywords: antimicrobial resistance; antimicrobials; nanopore sequencing; personalised dosing; sepsis diagnostics; trial protocol.
Copyright © 2021 Irwin, Coin, Harris, Cotta, Bauer, Buckley, Balch, Kruger, Meyer, Shekar, Brady, Fourie, Sharp, Vlad, Whiley, Beatson, Forde, Paterson, Clark, Hajkowicz, Raman, Bialasiewicz, Lipman, Schlapbach and Roberts.
Conflict of interest statement
AI has received research funding and teaching honoraria from Gilead Sciences inc. unrelated to this work. DP has received research funding from Pfizer, Merck and Shionogi and funding for advisory boards or speaking engagements from Merck, Pfizer, BioMerieux, Sumitomo, Accelerate, QPex and Entasis, unrelated to this work. LC has received research funding from Oxford Nanopore Technologies unrelated to this work, and received travel reimbursement to travel to a conference. JR has consulted for or received grants from The Medicines Company, MSD, Biomerieux, QPEX, Pfizer and Discuva. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Agyeman P. K. A., Schlapbach L. J., Giannoni E., Stocker M., Posfay-Barbe K. M., Heininger U., et al. . (2017). Epidemiology of Blood Culture-Proven Bacterial Sepsis in Children in Switzerland: A Population-Based Cohort Study. Lancet Child Adolesc. Health 1 (2), 124–133. 10.1016/S2352-4642(17)30010-X - DOI - PubMed
-
- Bialasiewicz S., Duarte T. P. S., Nguyen S. H., Sukumaran V., Stewart A., Appleton S., et al. . (2019). Rapid Diagnosis of Capnocytophaga Canimorsus Septic Shock in an Immunocompetent Individual Using Real-Time Nanopore Sequencing: A Case Report. BMC Infect. Dis. 19 (1), 660. 10.1186/s12879-019-4173-2 - DOI - PMC - PubMed
-
- Brenner T., Decker S. O., Grumaz S., Stevens P., Bruckner T., Schmoch T., et al. . (2018). Next-Generation Sequencing Diagnostics of Bacteremia in Sepsis (Next GeneSiS-Trial): Study Protocol of a Prospective, Observational, Noninterventional, Multicenter, Clinical Trial. Medicine 97 (6), e9868. 10.1097/MD.0000000000009868 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical