

Comparison of Residual Pulmonary Abnormalities 3 Months After Discharge in Patients Who Recovered From COVID-19 of Different Severity
- PMID: 34249973
- PMCID: PMC8270002
- DOI: 10.3389/fmed.2021.682087
Comparison of Residual Pulmonary Abnormalities 3 Months After Discharge in Patients Who Recovered From COVID-19 of Different Severity
Abstract
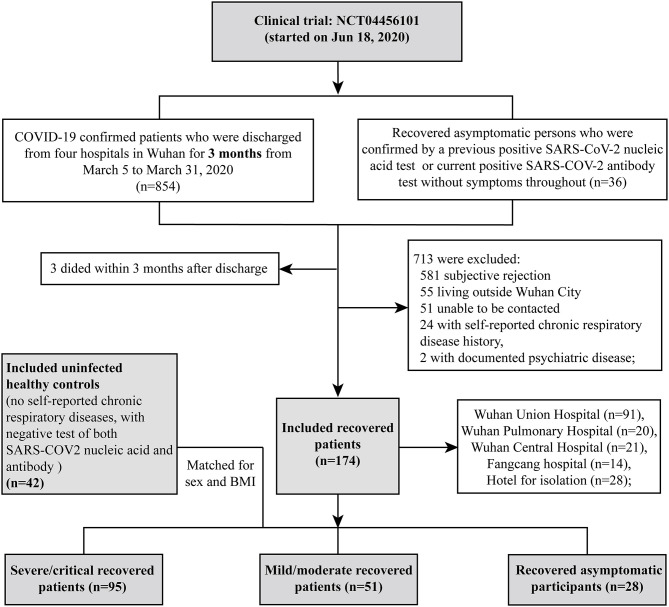
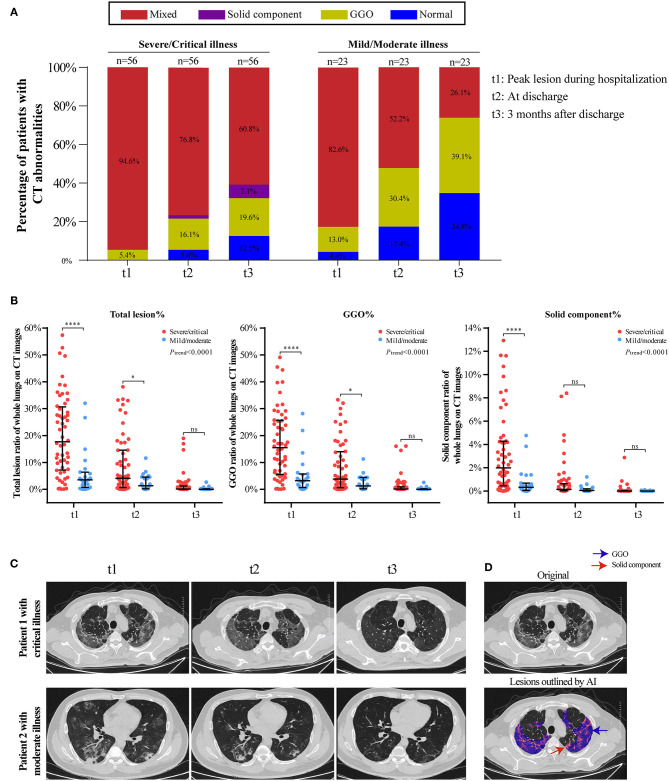
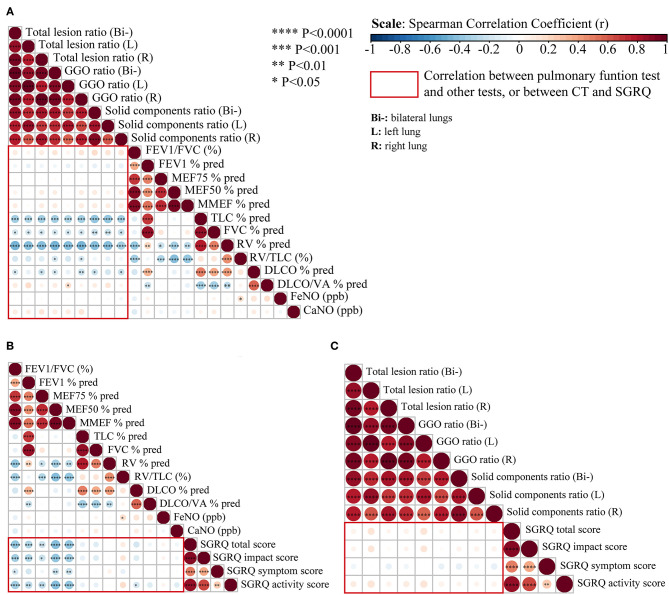
Background and Objectives: To investigate whether coronavirus disease 2019 (COVID-19) survivors who had different disease severities have different levels of pulmonary sequelae at 3 months post-discharge. Methods: COVID-19 patients discharged from four hospitals 3 months previously, recovered asymptomatic patients from an isolation hotel, and uninfected healthy controls (HCs) from the community were prospectively recruited. Participants were recruited at Wuhan Union Hospital and underwent examinations, including quality-of-life evaluation (St. George Respiratory Questionnaire [SGRQ]), laboratory examination, chest computed tomography (CT) imaging, and pulmonary function tests. Results: A total of 216 participants were recruited, including 95 patients who had recovered from severe/critical COVID-19 (SPs), 51 who had recovered from mild/moderate disease (MPs), 28 who had recovered from asymptomatic disease (APs), and 42 HCs. In total, 154 out of 174 (88.5%) recovered COVID-19 patients tested positive for serum SARS-COV-2 IgG, but only 19 (10.9%) were still positive for IgM. The SGRQ scores were highest in the SPs, while APs had slightly higher SGRQ scores than those of HCs; 85.1% of SPs and 68.0% of MPs still had residual CT abnormalities, mainly ground-glass opacity (GGO) followed by strip-like fibrosis at 3 months after discharge, but the pneumonic lesions were largely absorbed in the recovered SPs or MPs relative to findings in the acute phase. Pulmonary function showed that the frequency of lung diffusion capacity for carbon monoxide abnormalities were comparable in SPs and MPs (47.1 vs. 41.7%), while abnormal total lung capacity (TLC) and residual volume (RV) were more frequent in SPs than in MPs (TLC, 18.8 vs. 8.3%; RV, 11.8 vs. 0%). Conclusions: Pulmonary abnormalities remained after recovery from COVID-19 and were more frequent and conspicuous in SPs at 3 months after discharge.
Keywords: chest computerized tomography; health-related quality of life; laboratory findings; pulmonary function; recovered COVID-19 patients.
Copyright © 2021 Zhou, Xu, Liao, Yin, Yang, Wang, Wang, Yang, Wang, Peng, Peng, Wu, Chen and Jin.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- WHO . Coronavirus Disease (COVID-19) Dashboard. (2021). Available online at: https://covid19.who.int (accessed March 1, 2021).
LinkOut - more resources
Full Text Sources
Miscellaneous