

Performance and Operational Evaluation of the Access Bio CareStart Rapid Antigen Test in a High-Throughput Drive-Through Community Testing Site in Massachusetts
- PMID: 34250188
- PMCID: PMC8244626
- DOI: 10.1093/ofid/ofab243
Performance and Operational Evaluation of the Access Bio CareStart Rapid Antigen Test in a High-Throughput Drive-Through Community Testing Site in Massachusetts
Abstract
Background: To facilitate deployment of point-of-care testing for severe acute respiratory syndrome coronavirus 2, we evaluated the Access Bio CareStart COVID-19 Antigen test in a high-throughput, drive-through, free community testing site using anterior nasal (AN) swab reverse-transcription polymerase chain reaction (RT-PCR) for clinical testing.
Methods: Consenting symptomatic and asymptomatic children (≤18 years) and adults received dual AN swabs. CareStart testing was performed with temperature/humidity monitoring. All tests had 2 independent reads to assess interoperator agreement. Patients with positive CareStart results were called and instructed to isolate pending RT-PCR results. The paired RT-PCR result was the reference for sensitivity and specificity calculations.
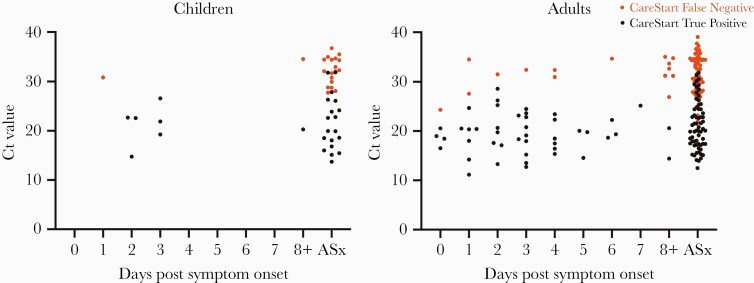
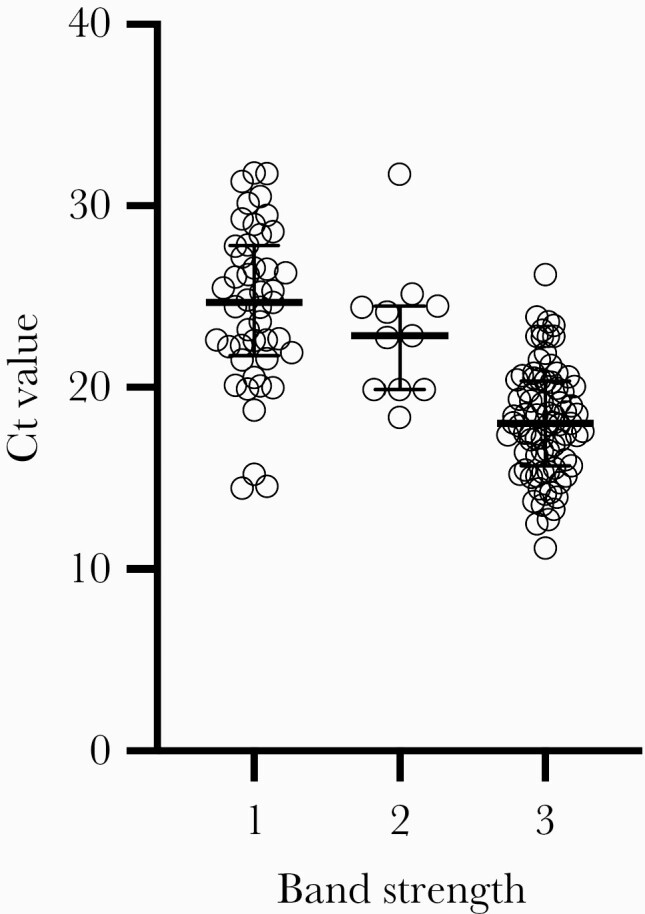
Results: Of 1603 participants, 1245 adults and 253 children had paired RT-PCR/CareStart results and complete symptom data. Eighty-three percent of adults and 87% of children were asymptomatic. CareStart sensitivity/specificity were 84.8% (95% confidence interval [CI], 71.1-93.7)/97.2% (95% CI, 92.0-99.4) and 85.7% (95% CI, 42.1-99.6)/89.5% (95% CI, 66.9-98.7) in adults and children, respectively, within 5 days of symptoms. Sensitivity/specificity were 50.0% (95% CI, 41.0-59.0)/99.1% (95% CI, 98.3-99.6) in asymptomatic adults and 51.4% (95% CI, 34.4-68.1)/97.8% (95% CI, 94.5-99.4) in asymptomatic children. Sensitivity in all 234 RT-PCR-positive people was 96.3% with cycle threshold (Ct) ≤25, 79.6% with Ct ≤30, and 61.4% with Ct ≤35. All 21 false-positive CareStart tests had faint but normal bands. Interoperator agreement was 99.5%. Operational challenges included identification of faint test bands and inconsistent swab elution volumes.
Conclusions: CareStart had high sensitivity in people with Ct ≤25 and moderate sensitivity in symptomatic people overall. Specificity was unexpectedly lower in symptomatic versus asymptomatic people. Excellent interoperator agreement was observed, but operational challenges indicate that operator training is warranted.
Keywords: COVID-19; SARS-CoV-2; antigen; diagnostic; point-of-care.
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Johns Hopkins University. COVID-19 dashboard by the center for systems science and engineering (CCSE) at Johns Hopkins University. Available at: https://coronavirus.jhu.edu/map.html. Accessed 12 February 2021.
-
- Centers for Disease Control. CDC COVID data tracker. Available at: https://covid.cdc.gov/covid-data-tracker/#testing_testsperformed. Accessed 12 February 2021.
-
- U.S. Food and Drug Administration. Individual EUAs for antigen diagnostic tests for SARS-CoV-2. Available at: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-em.... Accessed 10 February 2021.
-
- Krüger LJ, Gaeddert M, Köppel L, et al. Evaluation of the accuracy, ease of use and limit of detection of novel, rapid, antigen-detecting point-of-care diagnostics for SARS-CoV-2 [preprint ]. medRxiv 2020. doi: 10.1101/2020.10.01.20203836:2020.10.01.20203836. - DOI
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
