

Prediction of seizure recurrence risk following discontinuation of antiepileptic drugs
- PMID: 34250596
- PMCID: PMC8457060
- DOI: 10.1111/epi.16993
Prediction of seizure recurrence risk following discontinuation of antiepileptic drugs
Abstract
Objective: Discontinuation of antiepileptic drugs (AEDs) in seizure-free patients is an important goal because of possible long-term side effects and the social stigma burden of epilepsy. The purpose of this work was to assess seizure recurrence risk after suspension of AEDs, to evaluate predictors for recurrence, and to investigate the recovery of seizure control after relapse. In addition, the accuracy of a previously published prediction model of seizure recurrence risk was estimated.
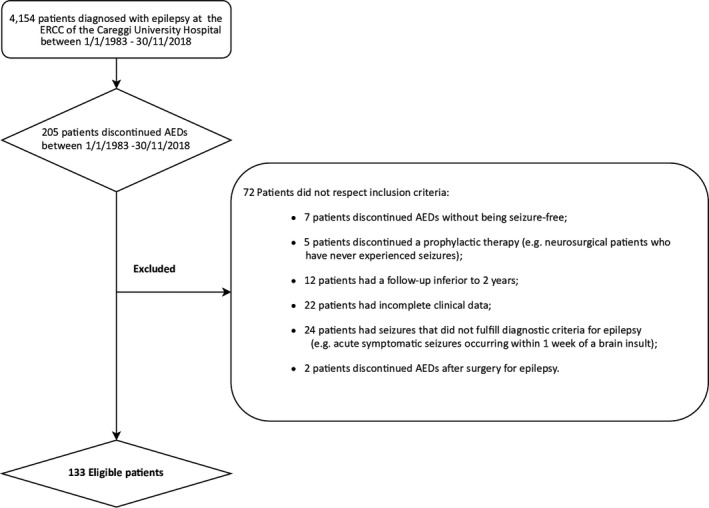
Methods: Seizure-free patients with epilepsy who had discontinued AEDs were retrospectively enrolled. The frequency of seizure relapses after AED withdrawal as well as prognosis after recurrence were assessed and the predictive role of baseline clinical-demographic variables was evaluated. The aforementioned prediction model was also validated and its accuracy assessed at different seizure-relapse probability levels.
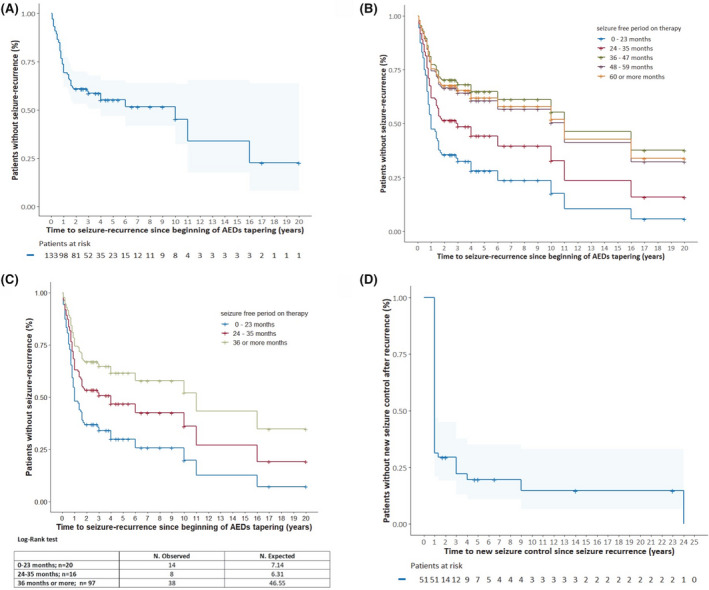
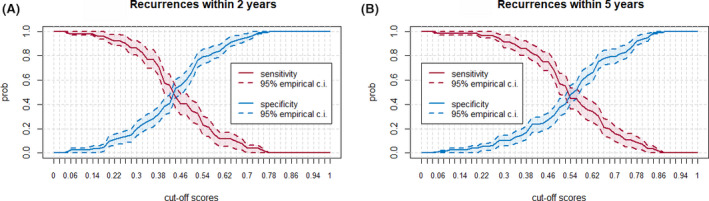
Results: The enrolled patients (n = 133) had been followed for a median of 3 years (range 0.8-33 years) after AED discontinuation; 60 (45%) of them relapsed. Previous febrile seizures in childhood (hazard ratio [HR] 3.927; 95% confidence interval [CI] 1.403-10.988), a seizure-free period on therapy of less than 2 years (HR 2.313; 95% CI 1.193-4.486), and persistent motor deficits (HR 4.568; 95% CI 1.412-14.772) were the clinical features associated with relapse risk in univariate analysis. Among these variables, only a seizure-free period on therapy of less than 2 years was associated with seizure recurrence in multivariate analysis (HR 2.365; 95% CI 1.178-4.7444). Pharmacological control of epilepsy was restored in 82.4% of the patients who relapsed. In this population, the aforementioned prediction model showed an unsatisfactory accuracy.
Significance: A period of freedom from seizure on therapy of less than 2 years was the main predictor of seizure recurrence. The accuracy of the previously described prediction tool was low in this cohort, thus suggesting its cautious use in real-world clinical practice.
Keywords: AED withdrawal; anti-seizure medications; epilepsy.
© 2021 The Authors. Epilepsia published by Wiley Periodicals LLC on behalf of International League Against Epilepsy.
Conflict of interest statement
Luca Massacesi, MD, received fees for participation in the advisory board, faculty of teaching courses, or scientific consultation from Novartis, Biogen, Roche, Mylan, Merck‐Serono, and Sanofi‐Genzyme. Educational grants were also received from Merck‐Serono, Teva, Sanofi‐Genzyme, Biogen, Novartis, Roche, and Mylan. Eleonora Rosati, MD, received fees for participation in advisory board or scientific consultation from Eisai, GW, Bial, and UCB. The remaining authors have no conflicts of interest to disclose.
Figures
Comment in
-
Is the crystal ball broken? Another external validation of the post-withdrawal seizure-relapse prediction model.Epilepsia. 2021 Dec;62(12):3146-3147. doi: 10.1111/epi.17096. Epub 2021 Oct 11. Epilepsia. 2021. PMID: 34633078 Free PMC article. No abstract available.
-
Response: Brightening the crystal ball: A constructive reappraisal of the postwithdrawal seizure relapse prediction model.Epilepsia. 2021 Dec;62(12):3148-3149. doi: 10.1111/epi.17095. Epub 2021 Oct 11. Epilepsia. 2021. PMID: 34633079 No abstract available.
References
-
- Lamberink HJ, Otte WM, Geerts AT, Pavlovic M, Ramos‐Lizana J, Marson AG, et al. Individualised prediction model of seizure recurrence and long‐term outcomes after withdrawal of antiepileptic drugs in seizure‐free patients: a systematic review and individual participant data meta‐analysis. Lancet Neurol. 2017;16:523–31. - PubMed
-
- Zou X, Hong Z, Chen J, Zhou D. Is antiepileptic drug withdrawal status related to quality of life in seizure‐free adult patients with epilepsy? Epilepsy Behav. 2014;31:129–35. - PubMed
