

Ct threshold values, a proxy for viral load in community SARS-CoV-2 cases, demonstrate wide variation across populations and over time
- PMID: 34250907
- PMCID: PMC8282332
- DOI: 10.7554/eLife.64683
Ct threshold values, a proxy for viral load in community SARS-CoV-2 cases, demonstrate wide variation across populations and over time
Abstract
Background: Information on SARS-CoV-2 in representative community surveillance is limited, particularly cycle threshold (Ct) values (a proxy for viral load).
Methods: We included all positive nose and throat swabs 26 April 2020 to 13 March 2021 from the UK's national COVID-19 Infection Survey, tested by RT-PCR for the N, S, and ORF1ab genes. We investigated predictors of median Ct value using quantile regression.
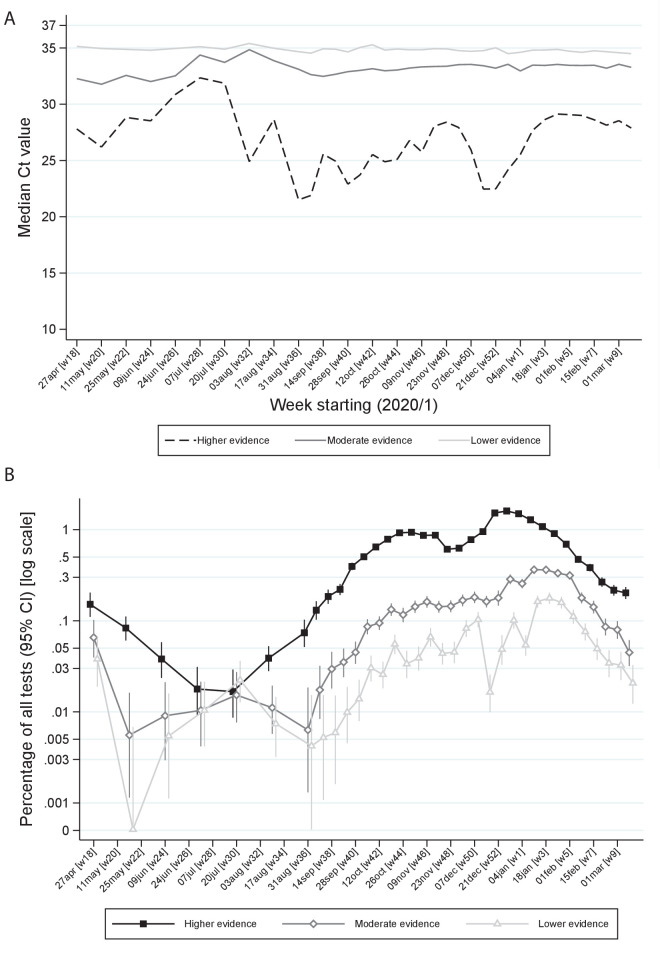
Results: Of 3,312,159 nose and throat swabs, 27,902 (0.83%) were RT-PCR-positive, 10,317 (37%), 11,012 (40%), and 6550 (23%) for 3, 2, or 1 of the N, S, and ORF1ab genes, respectively, with median Ct = 29.2 (~215 copies/ml; IQR Ct = 21.9-32.8, 14-56,400 copies/ml). Independent predictors of lower Cts (i.e. higher viral load) included self-reported symptoms and more genes detected, with at most small effects of sex, ethnicity, and age. Single-gene positives almost invariably had Ct > 30, but Cts varied widely in triple-gene positives, including without symptoms. Population-level Cts changed over time, with declining Ct preceding increasing SARS-CoV-2 positivity. Of 6189 participants with IgG S-antibody tests post-first RT-PCR-positive, 4808 (78%) were ever antibody-positive; Cts were significantly higher in those remaining antibody negative.
Conclusions: Marked variation in community SARS-CoV-2 Ct values suggests that they could be a useful epidemiological early-warning indicator.
Funding: Department of Health and Social Care, National Institutes of Health Research, Huo Family Foundation, Medical Research Council UK; Wellcome Trust.
Keywords: SARS-CoV-2; community; infectious disease; medicine; microbiology; symptoms; viral load.
© 2021, Walker et al.
Conflict of interest statement
AW, EP, TH, JR, PB, IB, JB, JN, JF, ID, RS, JH, KV, TP, NS, PM, KP No competing interests declared, DE declares lecture fees from Gilead, outside the submitted work.
Figures






References
-
- Buitrago-Garcia D, Egli-Gany D, Counotte MJ, Hossmann S, Imeri H, Ipekci AM, Salanti G, Low N. Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: a living systematic review and meta-analysis. PLOS Medicine. 2020;17:e1003346. doi: 10.1371/journal.pmed.1003346. - DOI - PMC - PubMed
-
- Byambasuren O, Cardona M, Bell K, Clark J, McLaws M-L, Glasziou P. Estimating the extent of asymptomatic COVID-19 and its potential for community transmission: systematic review and meta-analysis. Journal of the Association of Medical Microbiology and Infectious Disease Canada. 2020;5:223–234. doi: 10.3138/jammi-2020-0030. - DOI - PMC - PubMed
-
- Edwards T, Santos VS, Wilson AL, Cubas-Atienzar A. Variation of SARS-CoV-2 viral loads by sample type, disease severity and time: a systematic review. medRxiv. 2020 doi: 10.1101/2020.09.16.20195982. - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
