

Lopinavir-ritonavir and hydroxychloroquine for critically ill patients with COVID-19: REMAP-CAP randomized controlled trial
- PMID: 34251506
- PMCID: PMC8274471
- DOI: 10.1007/s00134-021-06448-5
Lopinavir-ritonavir and hydroxychloroquine for critically ill patients with COVID-19: REMAP-CAP randomized controlled trial
Abstract
Purpose: To study the efficacy of lopinavir-ritonavir and hydroxychloroquine in critically ill patients with coronavirus disease 2019 (COVID-19).
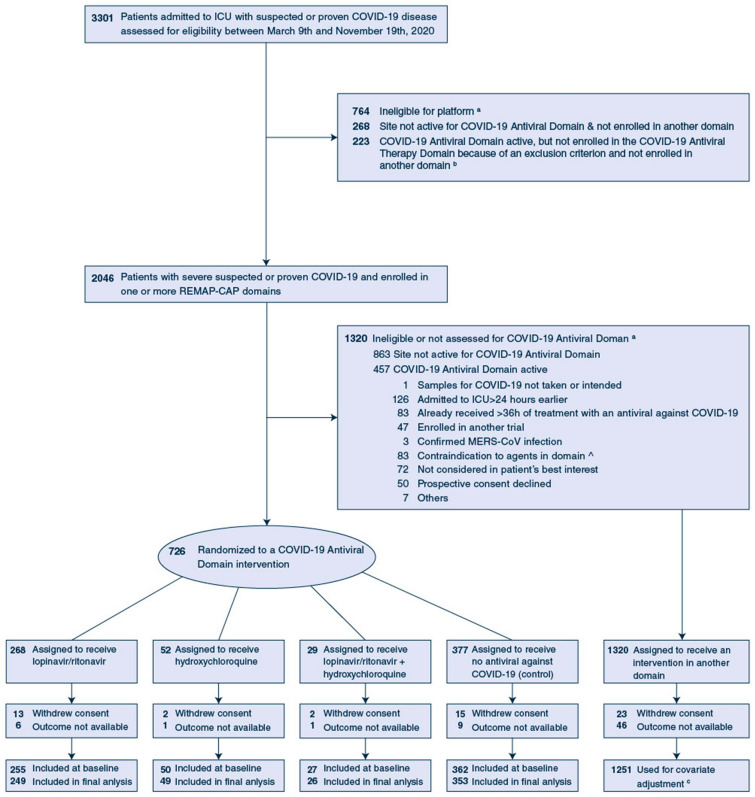
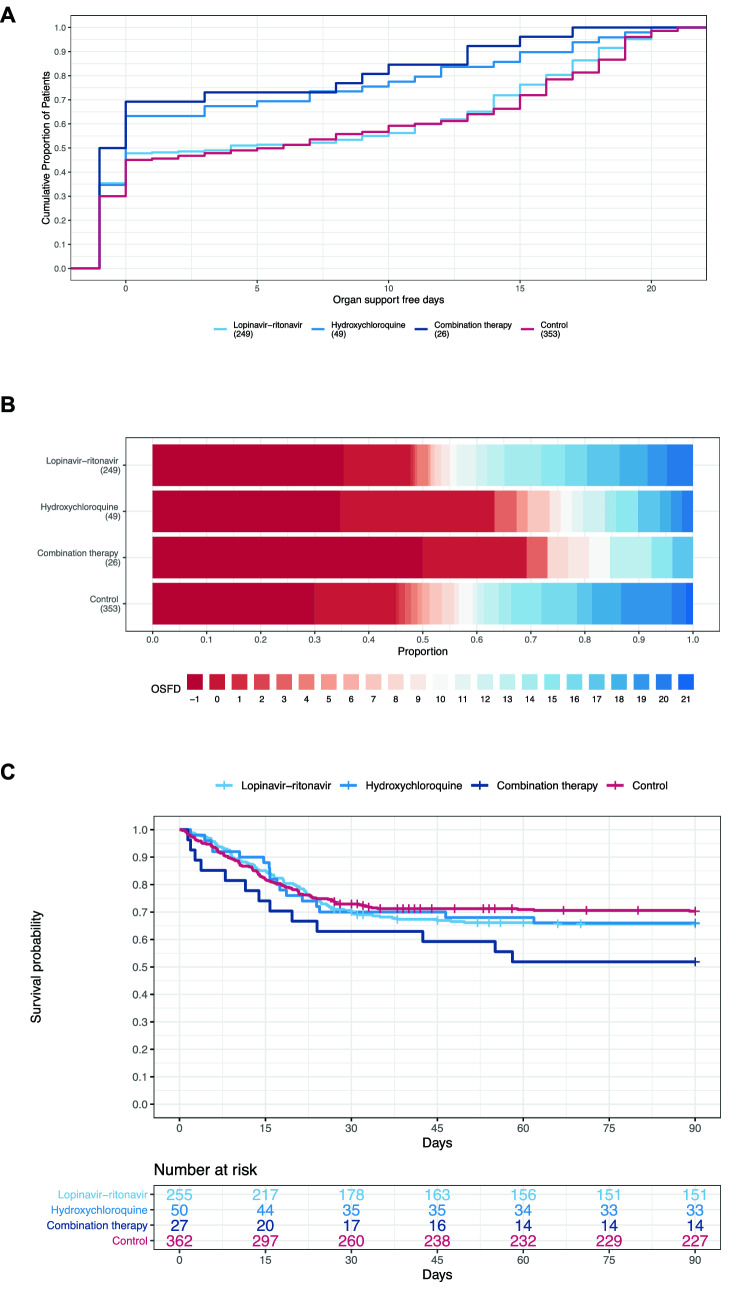
Methods: Critically ill adults with COVID-19 were randomized to receive lopinavir-ritonavir, hydroxychloroquine, combination therapy of lopinavir-ritonavir and hydroxychloroquine or no antiviral therapy (control). The primary endpoint was an ordinal scale of organ support-free days. Analyses used a Bayesian cumulative logistic model and expressed treatment effects as an adjusted odds ratio (OR) where an OR > 1 is favorable.
Results: We randomized 694 patients to receive lopinavir-ritonavir (n = 255), hydroxychloroquine (n = 50), combination therapy (n = 27) or control (n = 362). The median organ support-free days among patients in lopinavir-ritonavir, hydroxychloroquine, and combination therapy groups was 4 (- 1 to 15), 0 (- 1 to 9) and-1 (- 1 to 7), respectively, compared to 6 (- 1 to 16) in the control group with in-hospital mortality of 88/249 (35%), 17/49 (35%), 13/26 (50%), respectively, compared to 106/353 (30%) in the control group. The three interventions decreased organ support-free days compared to control (OR [95% credible interval]: 0.73 [0.55, 0.99], 0.57 [0.35, 0.83] 0.41 [0.24, 0.72]), yielding posterior probabilities that reached the threshold futility (≥ 99.0%), and high probabilities of harm (98.0%, 99.9% and > 99.9%, respectively). The three interventions reduced hospital survival compared with control (OR [95% CrI]: 0.65 [0.45, 0.95], 0.56 [0.30, 0.89], and 0.36 [0.17, 0.73]), yielding high probabilities of harm (98.5% and 99.4% and 99.8%, respectively).
Conclusion: Among critically ill patients with COVID-19, lopinavir-ritonavir, hydroxychloroquine, or combination therapy worsened outcomes compared to no antiviral therapy.
Trial registration: ClinicalTrials.gov NCT02735707.
Keywords: Adaptive platform trial; COVID-19; Hydroxychloroquine; Intensive care; Lopinavir-ritonavir; Pandemic; Pneumonia.
© 2021. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
ACG reports grants from NIHR, grants from NIHR Research Professorship (RP-2015-06-18), non-financial support from NIHR Clinical Research Network, during the conduct of the study; personal fees from GlaxoSmithKline, personal fees from Bristol Myers Squibb, personal fees from 30 Respiratory, outside the submitted work; LPGD is a member of the COVID-19 guideline committee SCCM/ESICM/SSC, member of the ESICM COVID-19 taskforce, and chair of the Dutch intensivists (NVIC) taskforce acute infectious threats; AND reports grants from Health Research Board of Ireland, during the conduct of the study; AB reports grants from Minderoo, grants from Wellcome, during the conduct of the study; LRB reports grants from EU PREPARE consortium, grants from Australian National Health and Medical Research Council, grants from Health Research Council of New Zealand, grants from UPMC, during the conduct of the study; CAB reports personal fees from BMS pfizer, non-financial support from Bayer, personal fees from Novartis, personal fees from Janssen, non-financial support from Amgen, personal fees from Lilly, personal fees from Portola, personal fees from Ablynx, outside the submitted work; MB reports other from Breast Cancer Research Foundation, during the conduct of the study; other from Eisai Inc, other from Amgen Inc, outside the submitted work; MDJ reports receiving fees for being on the Advisory Board for Roche and Cidara. He also reports receiving fee for being on IDSMB for Janssen and GSK; MAD reports grants from EU PREPARE, grants from Australian National Health and Medical Research Council, grants from Health Research Council of New Zealand, grants from UPMC, during the conduct of the study; MF reports grants from EU PREPARE, grants from Australian National Health and Medical Research Council, grants from Health Research Council of New Zealand, grants from UPMC, during the conduct of the study; RH reports grants from Wellcome Trust, during the conduct of the study; grants from National Institute of Health Research, outside the submitted work; AMH.reports grants from National Health and Medical Research Council and from the Minderoo Foundation during the conduct of the study; TEH. reports grants from Health Research Council of New Zealand, during the conduct of the study; CMH. reports grants from NICHD, during the conduct of the study; DTH.reports grants from The Breast Cancer Research Foundation in collaboration with the Translational Breast Cancer Research Consortium, during the conduct of the study; PRL. reports personal fees from Novartis, personal fees from Brigham and Women's Hospital, personal fees from Corona LLC, personal fees from McGraw Hill Publishing, outside the submitted work; RJL reports that Berry Consultants, LLC, a statistical consulting firm that specializes in the design, conduct, oversight, and analysis of adaptive and platform clinical trials, received support for its role in the design, conduct, and analysis of REMAP-CAP. Dr. Lewis is the Senior Medical Scientist at Berry Consultants, LLC; EL reports grants from EU, grants from Australian National Health and Medical Research Council, grants from Health Research Council of New Zealand, grants from UPMC, during the conduct of the study; DFM reports personal fees from consultancy for GlaxoSmithKline, Boehringer Ingelheim, Bayer, Novartis and Eli Lilly, and from sitting on a DMEC for a trial undertaken by Vir Biotechnology. In addition his institution has received funds from grants from several funders for studies in patients with ARDS and COVID-19. In addition, DFM has a patent (US8962032) issued to his institution for a treatment for inflammatory disease. He is a Director of Research for the Intensive Care Society and NIHR EME Programme Director; AM reports grants from EU-PREPARE, grants from Australian National Health and Medical Research Council, grants from Health Research Council of New Zealand, grants from UPMC, during the conduct of the study; B JM reports grants from Translational Breast Cancer Research Consortium, grants from UPMC Learning While Doing Program, during the conduct of the study; grants from NIH/NHLBI, grants from Bayer Pharmaceuticals, Inc, outside the submitted work; SCM reports grants from Health Research Council of New Zealand, during the conduct of the study; PRM reports grants from National Institute for Health Research, grants from European Union FP7 (PREPARE), during the conduct of the study; RP reports grants from Fisher and Paykel Healthcare NZ Ltd, outside the submitted work; KMR reports grants from European Union, grants from UK National Institute for Health Research, during the conduct of the study; CTS. reports grants from EU PREPARE, grants from Australian National Health and Medical Research Council, grants from Health Research Council of New Zealand, grants from UPMC, during the conduct of the study; CWS. reports grants from NIH, personal fees from Beckman Coulter, outside the submitted work; MSH reports other from National Institute For Health Research, outside the submitted work; AMT reports grants from Health Research Council of New Zealand, during the conduct of the study; FVV reports personal fees from Gilead, personal fees from Sobi, outside the submitted work; SB reports personal fees from Berry Consultants, during the conduct of the study; JCM. reports grants from Canadian Institutes of Health Research, during the conduct of the study; personal fees from Gilead Pharmaceuticals, outside the submitted work; CM reports grants from Health Research Council of New Zealand, non-financial support from Abbvie, during the conduct of the study; DCA reports non-financial support from European Union FP7 PREPARE, grants from Breast Cancer Research Foundation, Amgen, Inc., and Eisai, Inc, during the conduct of the study; SAW reports grants from National Health and Medical Research Council, grants from Minderoo Foundation, grants from Health Research Council, during the conduct of the study. *All other authors had no conflict of interest to disclose.
Figures
References
-
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard: https://covid19.who.int/?adgroupsurvey=%7Badgroupsurvey%7D&gclid=Cj0KCQj.... Acessed 11 June 2021
-
- de Wilde AH, Jochmans D, Posthuma CC, Zevenhoven-Dobbe JC, van Nieuwkoop S, Bestebroer TM, van den Hoogen BG, Neyts J, Snijder EJ. Screening of an FDA-approved compound library identifies four small-molecule inhibitors of Middle East respiratory syndrome coronavirus replication in cell culture. Antimicrob Agents Chemother. 2014;58:4875–4884. doi: 10.1128/AAC.03011-14. - DOI - PMC - PubMed
-
- Chan JF, Yao Y, Yeung ML, Deng W, Bao L, Jia L, Li F, Xiao C, Gao H, Yu P, Cai JP, Chu H, Zhou J, Chen H, Qin C, Yuen KY. Treatment with lopinavir/ritonavir or interferon-beta1b improves outcome of MERS-CoV infection in a nonhuman primate model of common marmoset. J Infect Dis. 2015;212:1904–1913. doi: 10.1093/infdis/jiv392. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
