

Neoadjuvant Treatment with Angiogenesis-Inhibitor Dovitinib Prior to Local Therapy in Hepatocellular Carcinoma: A Phase II Study
- PMID: 34251745
- PMCID: PMC8488766
- DOI: 10.1002/onco.13901
Neoadjuvant Treatment with Angiogenesis-Inhibitor Dovitinib Prior to Local Therapy in Hepatocellular Carcinoma: A Phase II Study
Abstract
Background: Hepatocellular carcinoma (HCC) recurrence rates following locoregional treatment are high. As multireceptor tyrosine kinase inhibitors targeting vascular endothelial growth factor receptors (VEGFRs) are effective in advanced HCC, we assessed the efficacy and safety of neoadjuvant systemic treatment with dovitinib in early- and intermediate-stage HCC.
Materials and methods: Twenty-four patients with modified Child-Pugh class A early- and intermediate-stage HCC received neoadjuvant oral dovitinib 500 mg daily (5 days on/2 days off) for 4 weeks, followed by locoregional therapy. Primary endpoints were objective response rates and intratumoral blood flow changes. Secondary endpoints were safety, pharmacodynamical plasma markers of VEGFR-blockade, time to progression (TTP), and overall survival (OS).
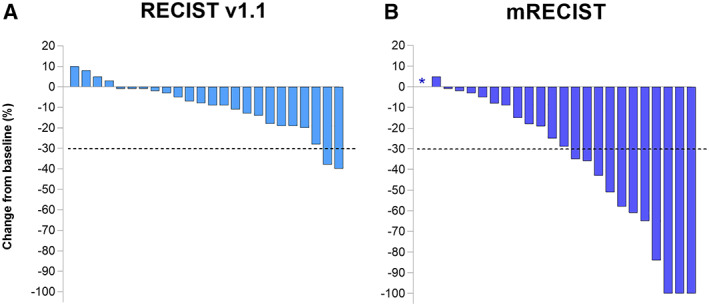
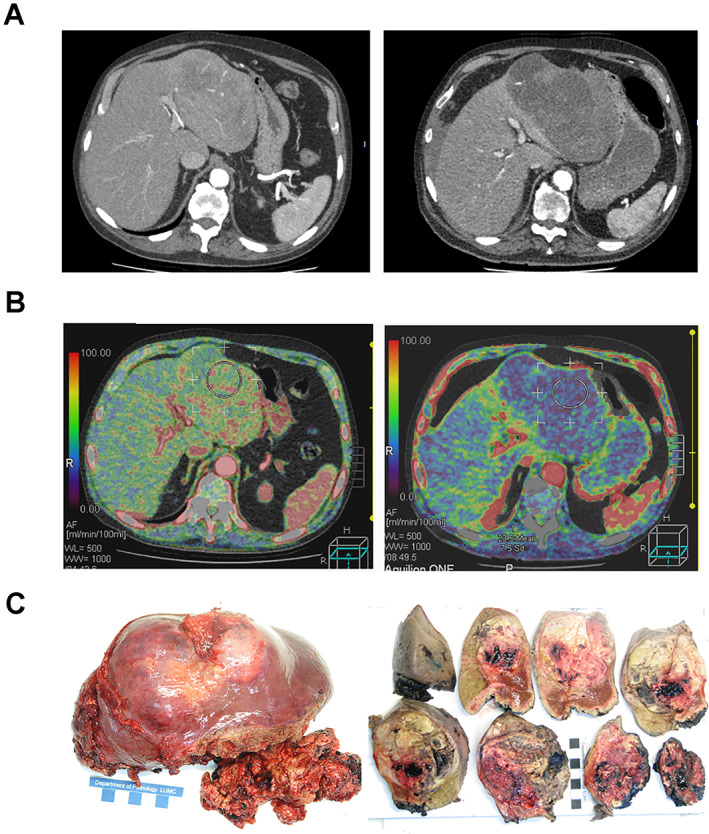
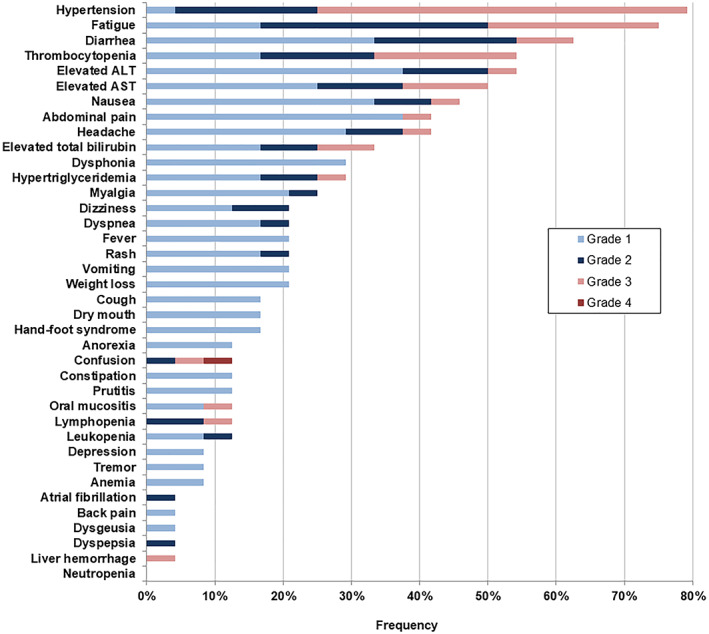
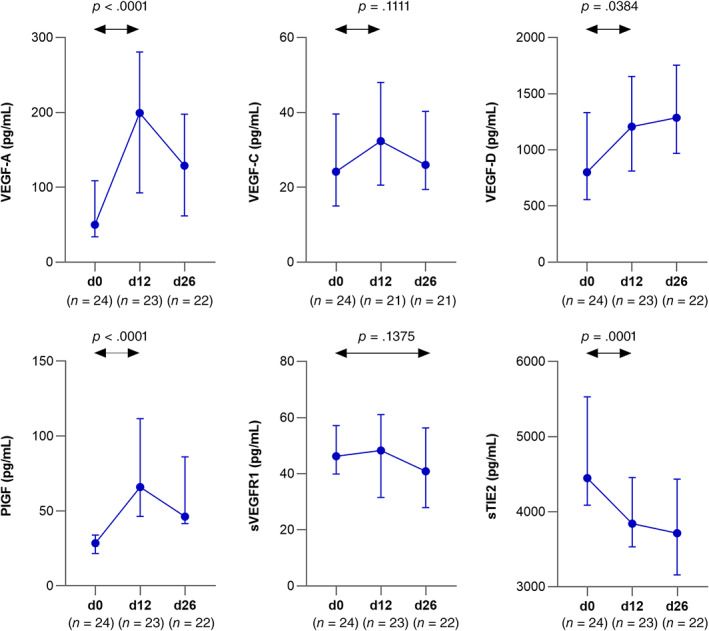
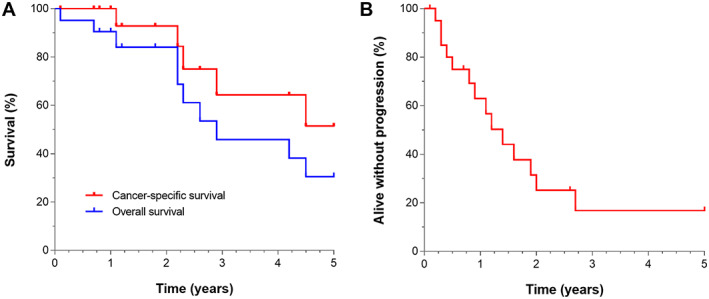
Results: Modified RECIST overall response rate was 48%, including 13% complete remission, and despite dose reduction/interruption in 83% of patients, intratumoral perfusion index decreased significantly. Grade 3-4 adverse events, most frequently (on-target) hypertension (54%), fatigue (25%), and thrombocytopenia (21%), occurred in 88% of patients. Plasma VEGF-A, VEGF-D, and placental growth factor increased significantly, whereas sTie-2 decreased, consistent with VEGFR-blockade. Following neoadjuvant dovitinib, all patients could proceed to their original planned locoregional treatment. No delayed toxicity occurred. Seven patients (three early, four intermediate stage) underwent orthotopic liver transplant after median 11.4 months. Censoring at transplantation, median TTP and OS were 16.8 and 34.8 months respectively; median cancer-specific survival was not reached.
Conclusion: Already after a short 4-week dovitinib treatment period, intratumoral blood flow reduction and modest antitumor responses were observed. Although these results support use of systemic neoadjuvant strategies, the poor tolerability indicates that dovitinib dose adaptations are required in HCC.
Implications for practice: Orthotopic liver transplantation may cure early and intermediate-stage hepatocellular carcinoma. Considering the expected waiting time >6 months because of donor liver scarcity, there is an unmet need for effective neoadjuvant downsizing strategies. Angiogenesis inhibition by dovitinib does not negatively affect subsequent invasive procedures, is safe to administer immediately before locoregional therapy, and may provide a novel treatment approach to improve patient outcomes if tolerability in patients with hepatocellular carcinoma can be improved by therapeutic drug monitoring and personalized dosing.
Keywords: Biomarker; Inflammation; Multireceptor tyrosine kinase inhibitor; Perfusion computed tomography; Quality of life.
© 2021 The Authors. The Oncologist published by Wiley Periodicals LLC on behalf of AlphaMed Press.
Conflict of interest statement
Figures
Comment in
-
Neoadjuvant Dovitinib in Early- and Intermediate-Stage Hepatocellular Carcinoma.Oncologist. 2022 Dec 9;27(12):e976. doi: 10.1093/oncolo/oyac168. Oncologist. 2022. PMID: 35993601 Free PMC article.
References
-
- Bray F, Ferlay J, Soerjomataram I et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018;68:394–424. - PubMed
-
- Vogel A, Cervantes A, Chau I et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow‐up. Ann Oncol 2018;29(suppl 4):iv238–iv255. - PubMed
-
- Finkenstedt A, Vikoler A, Portenkirchner M et al. Excellent post‐transplant survival in patients with intermediate stage hepatocellular carcinoma responding to neoadjuvant therapy. Liver Int 2016;36:688–695. - PubMed
-
- Doyle A, Gorgen A, Muaddi H et al. Outcomes of radiofrequency ablation as first‐line therapy for hepatocellular carcinoma less than 3cm in potentially transplantable patients. J Hepatol 2019;70:866–873. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
