

Operating in a Climate Crisis: A State-of-the-Science Review of Life Cycle Assessment within Surgical and Anesthetic Care
- PMID: 34251875
- PMCID: PMC8274692
- DOI: 10.1289/EHP8666
Operating in a Climate Crisis: A State-of-the-Science Review of Life Cycle Assessment within Surgical and Anesthetic Care
Abstract
Background: Both human health and the health systems we depend on are increasingly threatened by a range of environmental crises, including climate change. Paradoxically, health care provision is a significant driver of environmental pollution, with surgical and anesthetic services among the most resource-intensive components of the health system.
Objectives: This analysis aimed to summarize the state of life cycle assessment (LCA) practice as applied to surgical and anesthetic care via review of extant literature assessing environmental impacts of related services, procedures, equipment, and pharmaceuticals.
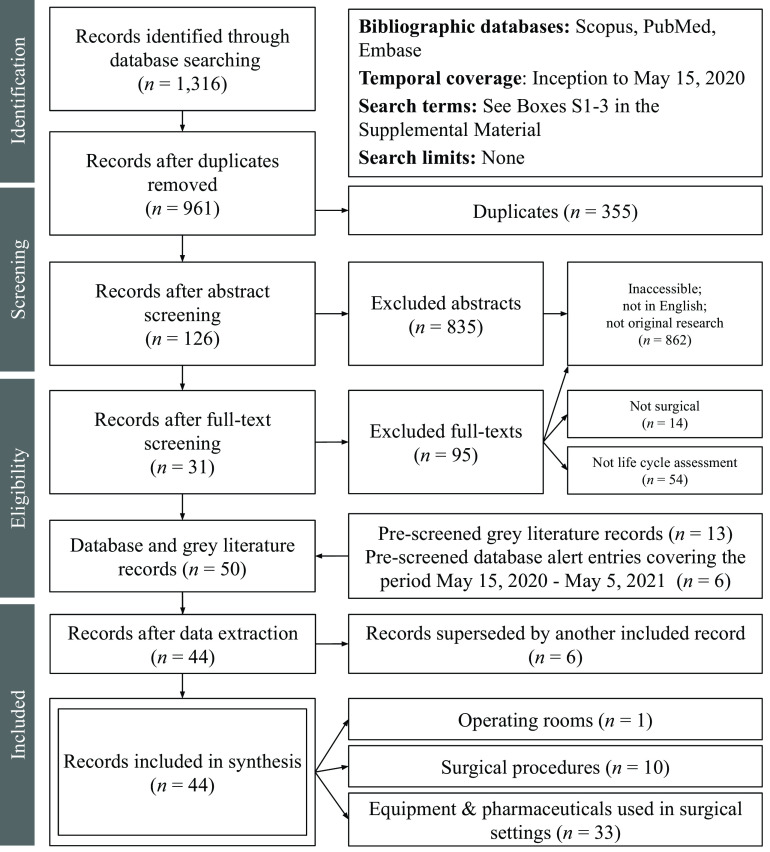
Methods: A state-of-the-science review was undertaken following a registered protocol and a standardized, LCA-specific reporting framework. Three bibliographic databases (Scopus®, PubMed, and Embase®) and the gray literature were searched. Inclusion criteria were applied, eligible entries critically appraised, and key methodological data and results extracted.
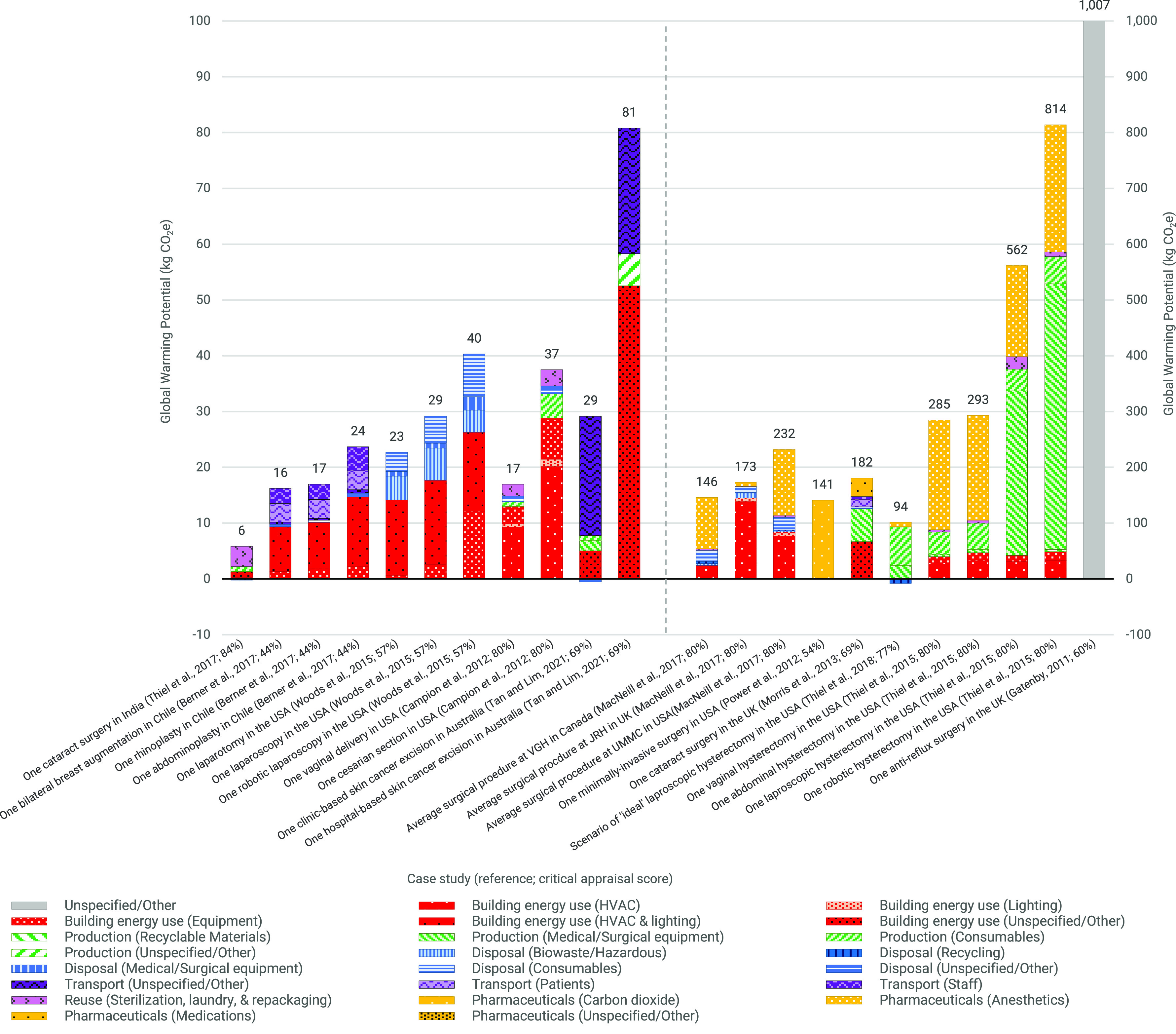
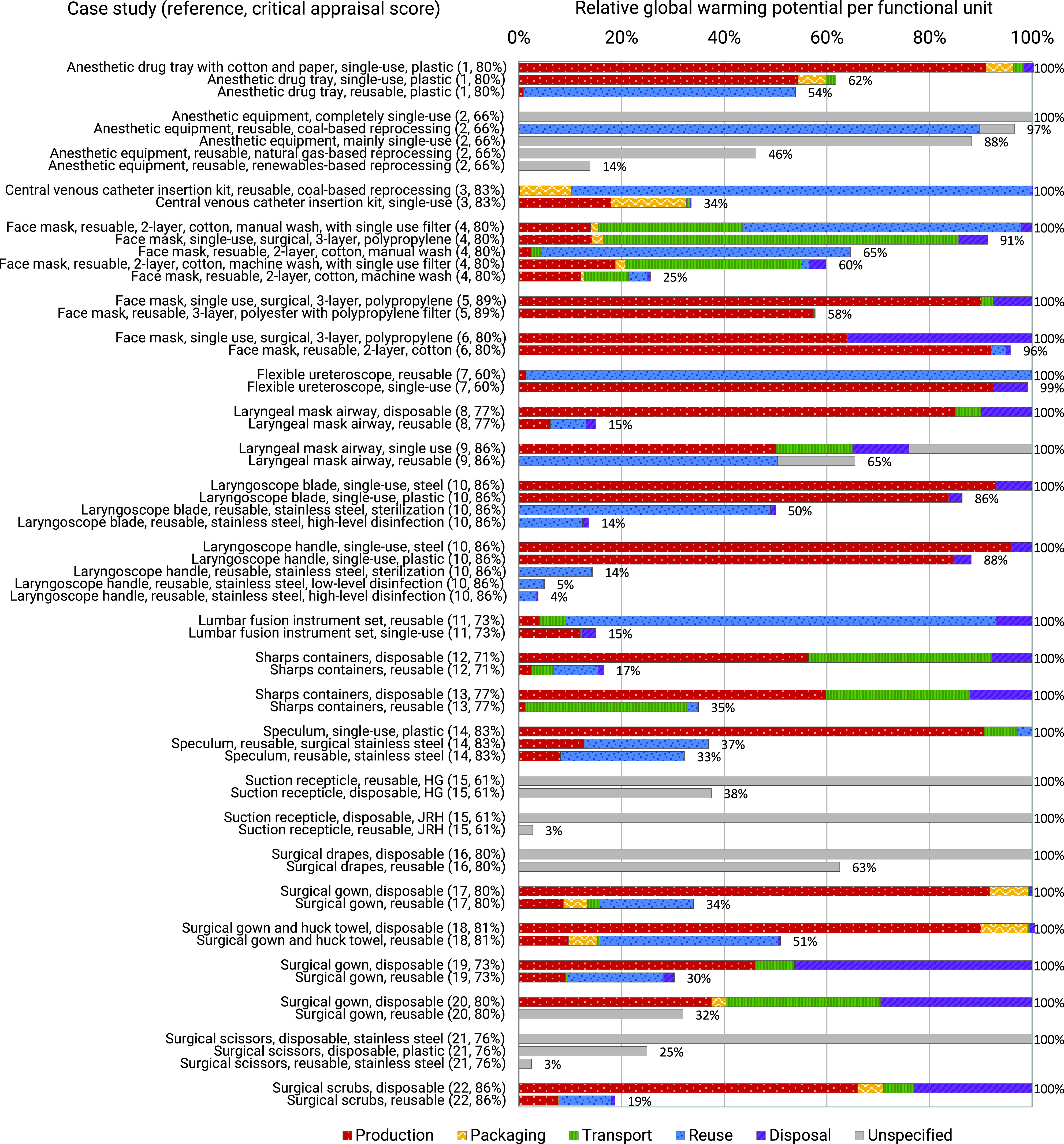
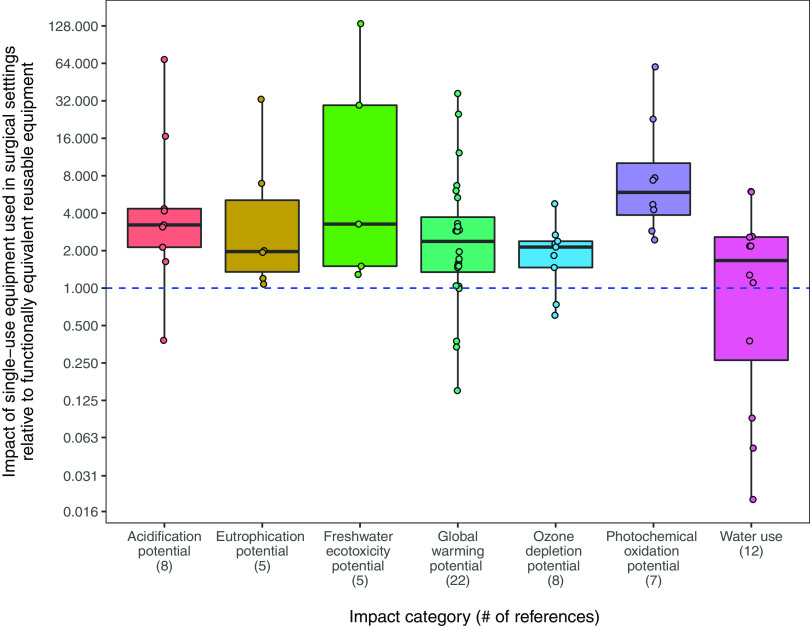
Results: From 1,316 identified records, 44 studies were eligible for inclusion. The annual climate impact of operating surgical suites ranged between 3,200,000 and . The climate impact of individual surgical procedures varied considerably, with estimates ranging from . Anesthetic gases; single-use equipment; and heating, ventilation, and air conditioning system operation were the main emissions hot spots identified among operating room- and procedure-specific analyses. Single-use equipment used in surgical settings was generally more harmful than equivalent reusable items across a range of environmental parameters. Life cycle inventories have been assembled and associated climate impacts calculated for three anesthetic gases () and 20 injectable anesthetic drugs ().
Discussion: Despite the recent proliferation of surgical and anesthesiology-related LCAs, extant studies address a miniscule fraction of the numerous services, procedures, and products available today. Methodological heterogeneity, external validity, and a lack of background life cycle inventory data related to many essential surgical and anesthetic inputs are key limitations of the current evidence base. This review provides an indication of the spectrum of environmental impacts associated with surgical and anesthetic care at various scales. https://doi.org/10.1289/EHP8666.
Figures
Comment in
-
Invited Perspective: Life Cycle Analysis: A Potentially Transformative Tool for Lowering Health Care's Carbon Footprint.Environ Health Perspect. 2021 Jul;129(7):71302. doi: 10.1289/EHP9630. Epub 2021 Jul 12. Environ Health Perspect. 2021. PMID: 34251876 Free PMC article. No abstract available.
References
-
- Allison AL, Ambrose-Dempster E, Domenech Aparsi T, Bawn M, Casas Arredondo M, Chau C, et al. . 2020. The environmental dangers of employing single-use face masks as part of a COVID-19 exit strategy. UCL Open: Environment Preprint. 10.14324/111.444/000031.v1, [accessed 25 July 2020]. - DOI
-
- Alshqaqeeq F, Esmaeili MA, Overcash M, Twomey J. 2020. Quantifying hospital services by carbon footprint: a systematic literature review of patient care alternatives. Resour Conserv Recycl 154:104560, 10.1016/j.resconrec.2019.104560. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
