

Why Remdesivir Failed: Preclinical Assumptions Overestimate the Clinical Efficacy of Remdesivir for COVID-19 and Ebola
- PMID: 34252308
- PMCID: PMC8448091
- DOI: 10.1128/AAC.01117-21
Why Remdesivir Failed: Preclinical Assumptions Overestimate the Clinical Efficacy of Remdesivir for COVID-19 and Ebola
Abstract
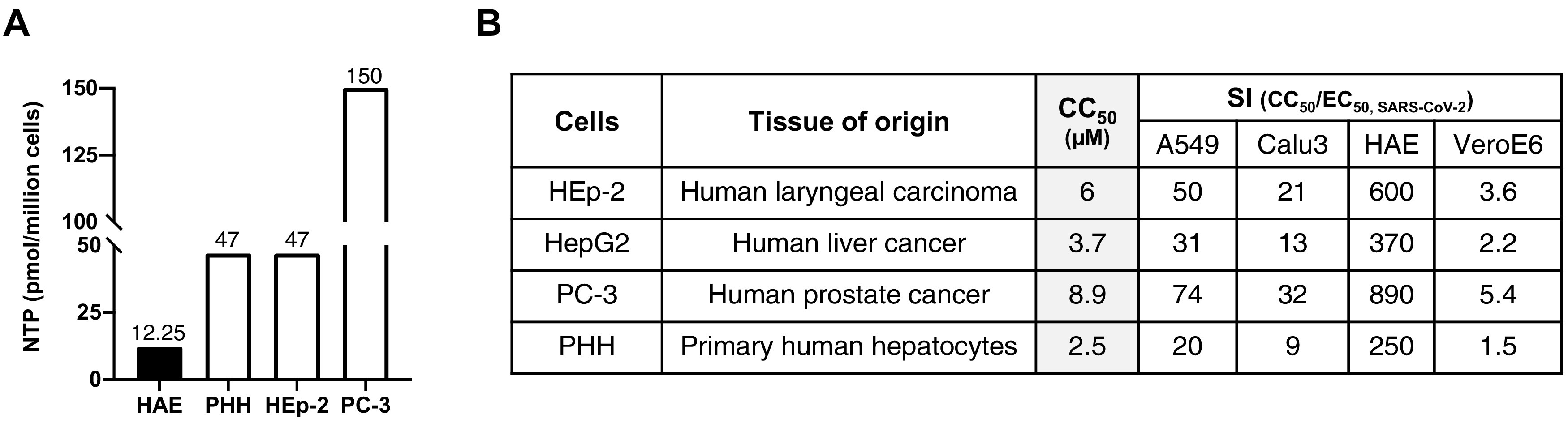
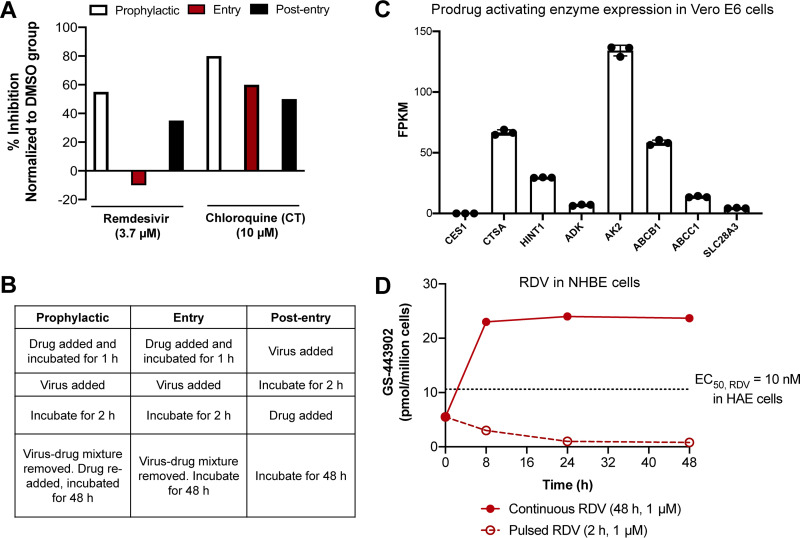
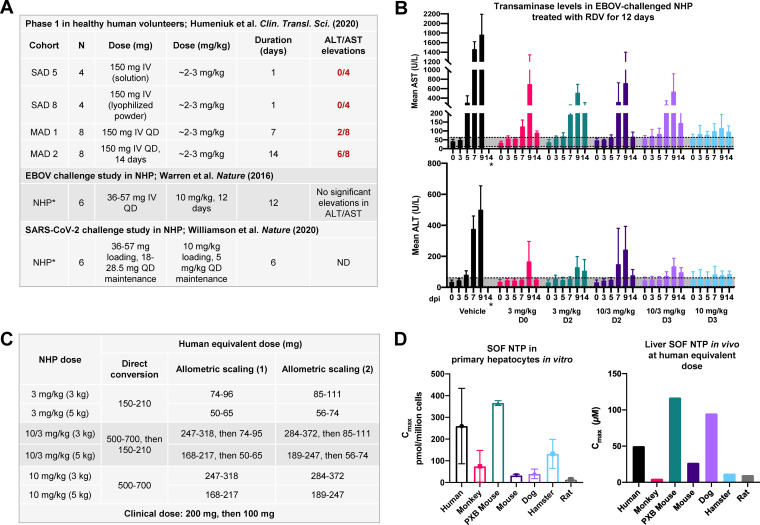
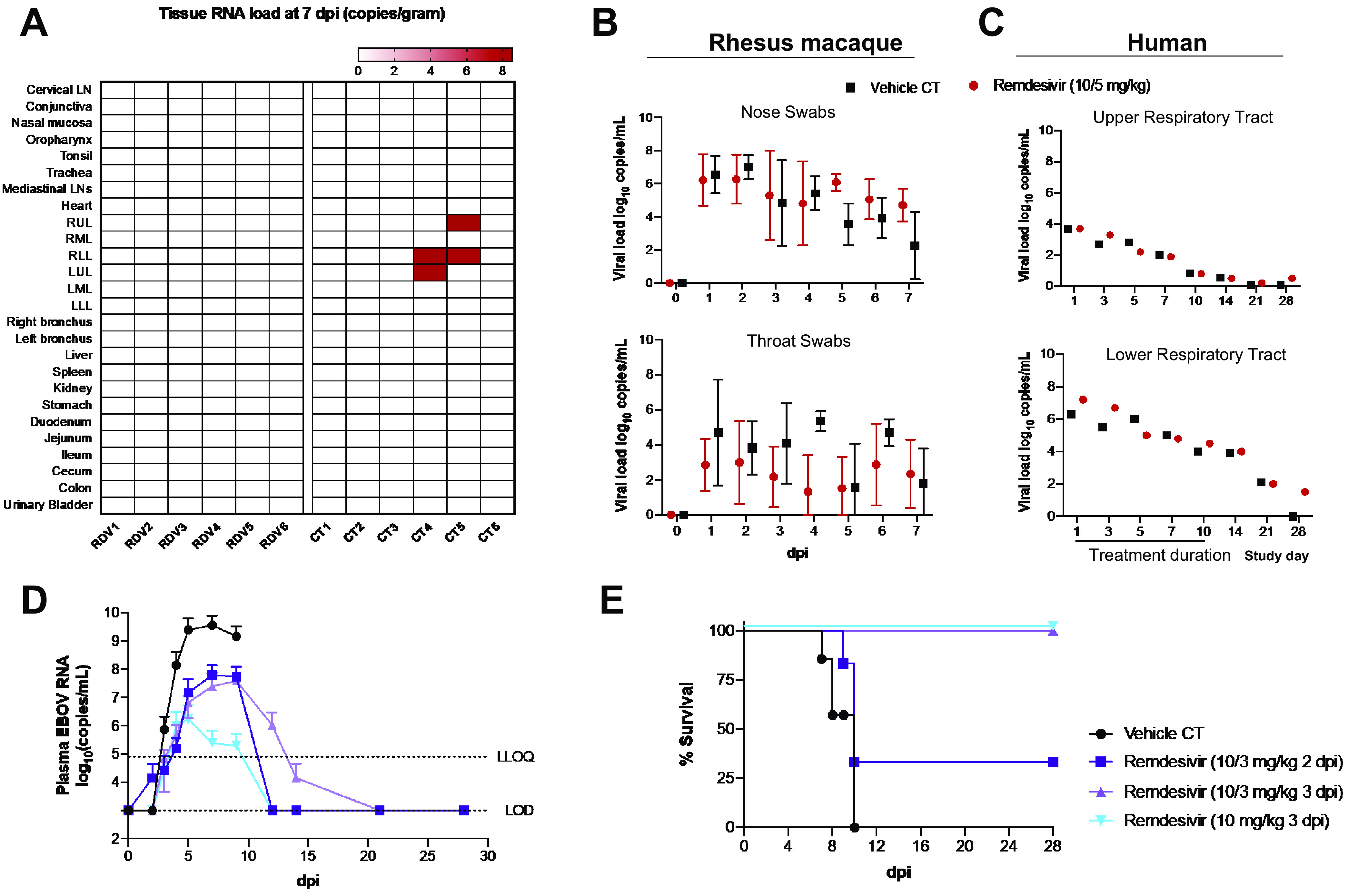
Remdesivir is a nucleoside monophosphoramidate prodrug that has been FDA approved for coronavirus disease 2019 (COVID-19). However, the clinical efficacy of remdesivir for COVID-19 remains contentious, as several trials have not found statistically significant differences in either time to clinical improvement or mortality between remdesivir-treated and control groups. Similarly, the inability of remdesivir to provide a clinically significant benefit above other investigational agents in patients with Ebola contrasts with strong, curative preclinical data generated in rhesus macaque models. For both COVID-19 and Ebola, significant discordance between the robust preclinical data and remdesivir's lackluster clinical performance have left many puzzled. Here, we critically evaluate the assumptions of the models underlying remdesivir's promising preclinical data and show that such assumptions overpredict efficacy and minimize toxicity of remdesivir in humans. Had the limitations of in vitro drug efficacy testing and species differences in drug metabolism been considered, the underwhelming clinical performance of remdesivir for both COVID-19 and Ebola would have been fully anticipated.
Keywords: GS-441524; GS-5734; in vitro models; in vivo models; nonhuman primates; pharmacokinetics; prodrug; remdesivir.
Figures
Similar articles
-
Remdesivir: A beacon of hope from Ebola virus disease to COVID-19.Rev Med Virol. 2020 Nov;30(6):1-13. doi: 10.1002/rmv.2133. Epub 2020 Jul 30. Rev Med Virol. 2020. PMID: 33210457 Review.
-
Broad-Spectrum In Vitro Antiviral Activity of ODBG-P-RVn: An Orally-Available, Lipid-Modified Monophosphate Prodrug of Remdesivir Parent Nucleoside (GS-441524).Microbiol Spectr. 2021 Dec 22;9(3):e0153721. doi: 10.1128/Spectrum.01537-21. Epub 2021 Nov 24. Microbiol Spectr. 2021. PMID: 34817209 Free PMC article.
-
Remdesivir: From Ebola to COVID-19.Biochem Biophys Res Commun. 2021 Jan 29;538:145-150. doi: 10.1016/j.bbrc.2020.11.043. Epub 2020 Nov 19. Biochem Biophys Res Commun. 2021. PMID: 33388129 Free PMC article. Review.
-
Development and validation of a UHPLC-MS/MS method for quantification of the prodrug remdesivir and its metabolite GS-441524: a tool for clinical pharmacokinetics of SARS-CoV-2/COVID-19 and Ebola virus disease.J Antimicrob Chemother. 2020 Jul 1;75(7):1772-1777. doi: 10.1093/jac/dkaa152. J Antimicrob Chemother. 2020. PMID: 32361744 Free PMC article.
-
The development of broad-spectrum antiviral medical countermeasures to treat viral hemorrhagic fevers caused by natural or weaponized virus infections.PLoS Negl Trop Dis. 2022 Mar 8;16(3):e0010220. doi: 10.1371/journal.pntd.0010220. eCollection 2022 Mar. PLoS Negl Trop Dis. 2022. PMID: 35259154 Free PMC article. Review.
Cited by
-
Lancemaside A from Codonopsis lanceolata: Studies on Antiviral Activity and Mechanism of Action against SARS-CoV-2 and Its Variants of Concern.Antimicrob Agents Chemother. 2022 Dec 20;66(12):e0120122. doi: 10.1128/aac.01201-22. Epub 2022 Nov 14. Antimicrob Agents Chemother. 2022. PMID: 36374087 Free PMC article.
-
Analyzing the Difference in the Length of Stay (LOS) in Moderate to Severe COVID-19 Patients Receiving Hydroxychloroquine or Favipiravir.Pharmaceuticals (Basel). 2022 Nov 24;15(12):1456. doi: 10.3390/ph15121456. Pharmaceuticals (Basel). 2022. PMID: 36558907 Free PMC article.
-
What Should Be Learned From Repurposed Antivirals Against SARS-CoV-2?Front Microbiol. 2022 Feb 16;13:843587. doi: 10.3389/fmicb.2022.843587. eCollection 2022. Front Microbiol. 2022. PMID: 35250956 Free PMC article. No abstract available.
-
Population Pharmacokinetics of Remdesivir and GS-441524 in Hospitalized COVID-19 Patients.Antimicrob Agents Chemother. 2022 Jun 21;66(6):e0025422. doi: 10.1128/aac.00254-22. Epub 2022 Jun 1. Antimicrob Agents Chemother. 2022. PMID: 35647646 Free PMC article.
-
Clinical pharmacodynamics of obeldesivir versus remdesivir.Antimicrob Agents Chemother. 2024 Sep 4;68(9):e0096924. doi: 10.1128/aac.00969-24. Epub 2024 Aug 12. Antimicrob Agents Chemother. 2024. PMID: 39133123 Free PMC article. No abstract available.
References
-
- Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, Hohmann E, Chu HY, Luetkemeyer A, Kline S, Lopez de Castilla D, Finberg RW, Dierberg K, Tapson V, Hsieh L, Patterson TF, Paredes R, Sweeney DA, Short WR, Touloumi G, Lye DC, Ohmagari N, Oh M, Ruiz-Palacios GM, Benfield T, Fätkenheuer G, Kortepeter MG, Atmar RL, Creech CB, Lundgren J, Babiker AG, Pett S, Neaton JD, Burgess TH, Bonnett T, Green M, Makowski M, Osinusi A, Nayak S, Lane HC. 2020. Remdesivir for the treatment of Covid-19—final report. N Engl J Med 383:1813–1826. 10.1056/NEJMoa2007764. - DOI - PMC - PubMed
-
- Wang Y, Zhang D, Du G, Du R, Zhao J, Jin Y, Fu S, Gao L, Cheng Z, Lu Q, Hu Y, Luo G, Wang K, Lu Y, Li H, Wang S, Ruan S, Yang C, Mei C, Wang Y, Ding D, Wu F, Tang X, Ye X, Ye Y, Liu B, Yang J, Yin W, Wang A, Fan G, Zhou F, Liu Z, Gu X, Xu J, Shang L, Zhang Y, Cao L, Guo T, Wan Y, Qin H, Jiang Y, Jaki T, Hayden FG, Horby PW, Cao B, Wang C. 2020. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet 395:1569–1578. 10.1016/S0140-6736(20)31022-9. - DOI - PMC - PubMed
-
- WHO. 2020. WHO recommends against the use of remdesivir in COVID-19 patients.
-
- Pruijssers AJ, George AS, Schäfer A, Leist SR, Gralinksi LE, Dinnon KH, Yount BL, Agostini ML, Stevens LJ, Chappell JD, Lu X, Hughes TM, Gully K, Martinez DR, Brown AJ, Graham RL, Perry JK, Du Pont V, Pitts J, Ma B, Babusis D, Murakami E, Feng JY, Bilello JP, Porter DP, Cihlar T, Baric RS, Denison MR, Sheahan TP. 2020. Remdesivir inhibits SARS-CoV-2 in human lung cells and chimeric SARS-CoV expressing the SARS-CoV-2 RNA polymerase in mice. Cell Rep 32:107940. 10.1016/j.celrep.2020.107940. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
