

Comparing the downstream costs and healthcare utilization associated with the use of low-dose computed tomography (LDCT) in lung cancer screening in patients with and without alzheimer's disease and related dementias (ADRD)
- PMID: 34252317
- PMCID: PMC8627644
- DOI: 10.1080/03007995.2021.1953972
Comparing the downstream costs and healthcare utilization associated with the use of low-dose computed tomography (LDCT) in lung cancer screening in patients with and without alzheimer's disease and related dementias (ADRD)
Abstract
Objective: This study aims to compare the downstream costs and healthcare utilization associated with using low-dose computed tomography (LDCT) for lung cancer screening in patients with and without Alzheimer's disease and related dementias (ADRD).
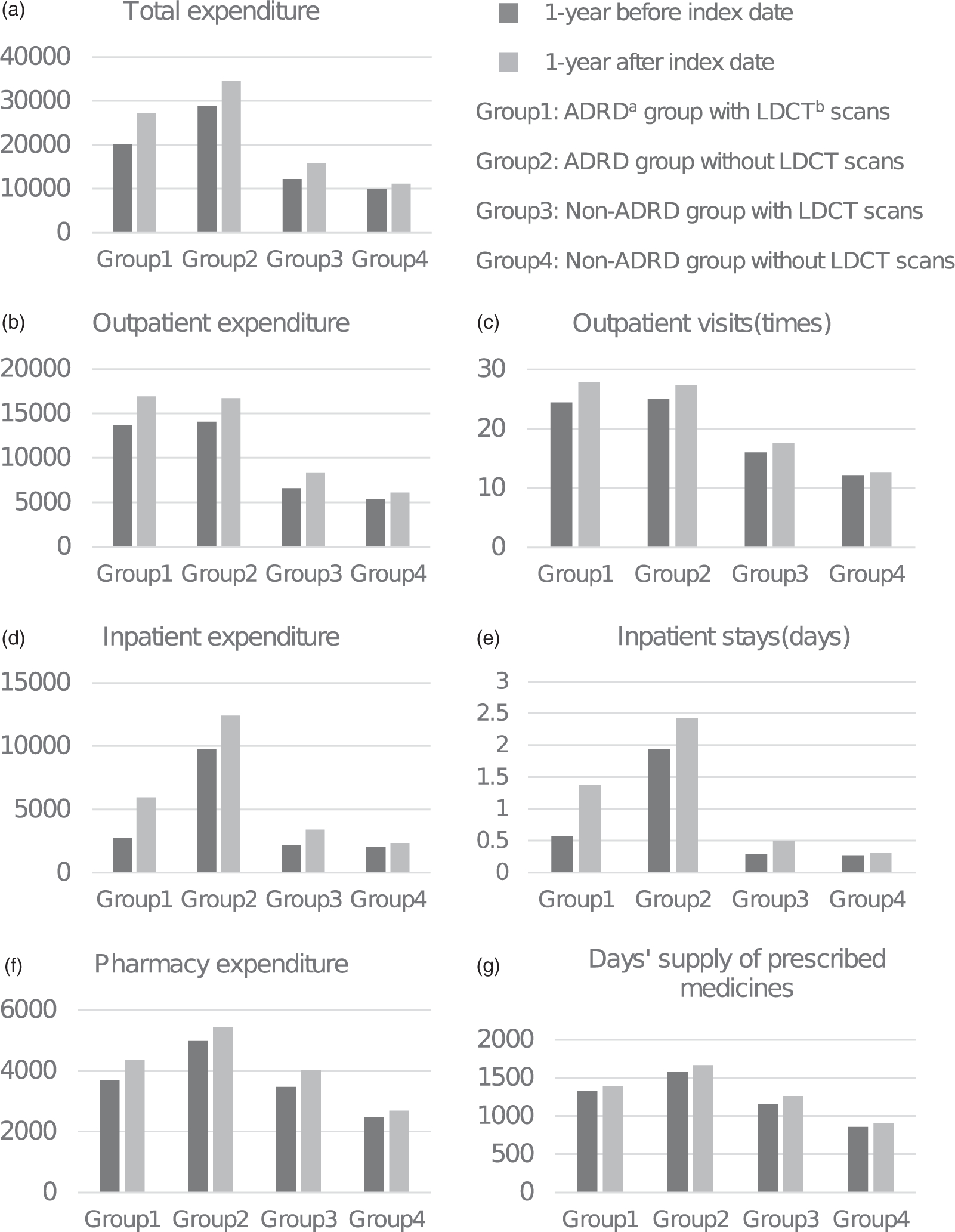
Methods: Based on data from IBM MarketScan Commercial Claims Databases (2014-2018), we have identified four study cohorts: ADRD and non-ADRD patients who went through LDCT screening; ADRD and non-ADRD patients without LDCT screening. Annually healthcare utilization and cost were grouped into outpatient, inpatient, and pharmacy. We used difference-in-differences (DID) models to estimate the downstream healthcare utilization and cost associated with LDCT screening in both ADRD and non-ADRD population. We used a difference-in-difference-in-differences (DDD) model to explore whether LDCT screening was associated with higher downstream cost and healthcare utilization in ADRD population than non-ADRD population.
Result: Compared to individuals without LDCT screening, LDCT screening was associated with increased outpatient visits (2.1, 95% CI 0.7, 3.4) and outpatient cost ($2301.0, 95% CI 296.2, 4305.8) in the ADRD population and increased outpatient visits (0.6, 95% CI 0.1, 1.1) in the non-ADRD population within 1 year after screening. Compared with the non-ADRD population, LDCT screening was found to be associated with an additional 1.5 (95% CI 0.2, 2.8) outpatient visits, 0.7 (95% CI 0.1, 1.3) days of inpatient stays, and $4,960.4 (95% CI 532.7, 9388.0) in overall healthcare costs within 1-year after LDCT in the ADRD population (all p < .5).
Conclusion: The downstream cost and healthcare utilization associated with LDCT screening were found to be higher in the ADRD population compared to the average population.
Keywords: Alzheimer’s disease and related dementias; Lung cancer screening; expenditures; healthcare utilization; low-dose computed tomography.
Figures
Similar articles
-
Lung cancer screening with low-dose computed tomography: National expenditures and cost-effectiveness.Front Public Health. 2022 Sep 29;10:977550. doi: 10.3389/fpubh.2022.977550. eCollection 2022. Front Public Health. 2022. PMID: 36249202 Free PMC article.
-
Health Care Utilization, Care Satisfaction, and Health Status for Medicare Advantage and Traditional Medicare Beneficiaries With and Without Alzheimer Disease and Related Dementias.JAMA Netw Open. 2020 Mar 2;3(3):e201809. doi: 10.1001/jamanetworkopen.2020.1809. JAMA Netw Open. 2020. PMID: 32227181 Free PMC article.
-
Wisconsin Healthcare Utilization Cost Among American Indians/Alaska Natives with and without Alzheimer's Disease and Related Dementias.J Alzheimers Dis. 2023;91(1):183-189. doi: 10.3233/JAD-220393. J Alzheimers Dis. 2023. PMID: 36373315 Free PMC article.
-
Population-Based Screening Using Low-Dose Chest Computed Tomography: A Systematic Review of Health Economic Evaluations.Pharmacoeconomics. 2023 Apr;41(4):395-411. doi: 10.1007/s40273-022-01238-3. Epub 2023 Jan 20. Pharmacoeconomics. 2023. PMID: 36670332 Free PMC article.
-
Lung cancer screening with low-dose computed tomography: costs, national expenditures, and cost-effectiveness.J Natl Compr Canc Netw. 2012 Feb;10(2):267-75. doi: 10.6004/jnccn.2012.0023. J Natl Compr Canc Netw. 2012. PMID: 22308519 Review.
Cited by
-
The Impact of Race-Ethnicity and Diagnosis of Alzheimer's Disease and Related Dementias on Mammography Use.Cancers (Basel). 2022 Sep 28;14(19):4726. doi: 10.3390/cancers14194726. Cancers (Basel). 2022. PMID: 36230648 Free PMC article.
References
-
- WHO. Cancer today. CANCER FACT SHEETS. http://gco.iarc.fr/today/home.
-
- Cancer of the Lung and Bronchus - Cancer Stat Facts. SEER Web site. https://seer.cancer.gov/statfacts/html/lungb.html
-
- Moyer VA US Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330–338. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials