

Individualized resuscitation strategy for septic shock formalized by finite mixture modeling and dynamic treatment regimen
- PMID: 34253228
- PMCID: PMC8273991
- DOI: 10.1186/s13054-021-03682-7
Individualized resuscitation strategy for septic shock formalized by finite mixture modeling and dynamic treatment regimen
Abstract
Background: Septic shock comprises a heterogeneous population, and individualized resuscitation strategy is of vital importance. The study aimed to identify subclasses of septic shock with non-supervised learning algorithms, so as to tailor resuscitation strategy for each class.
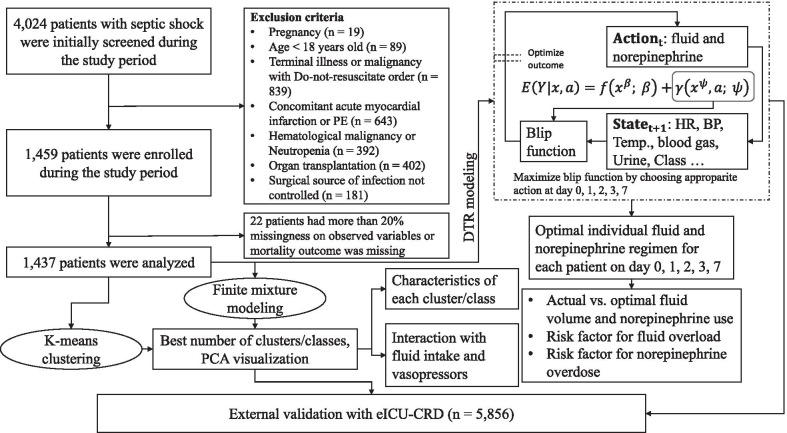
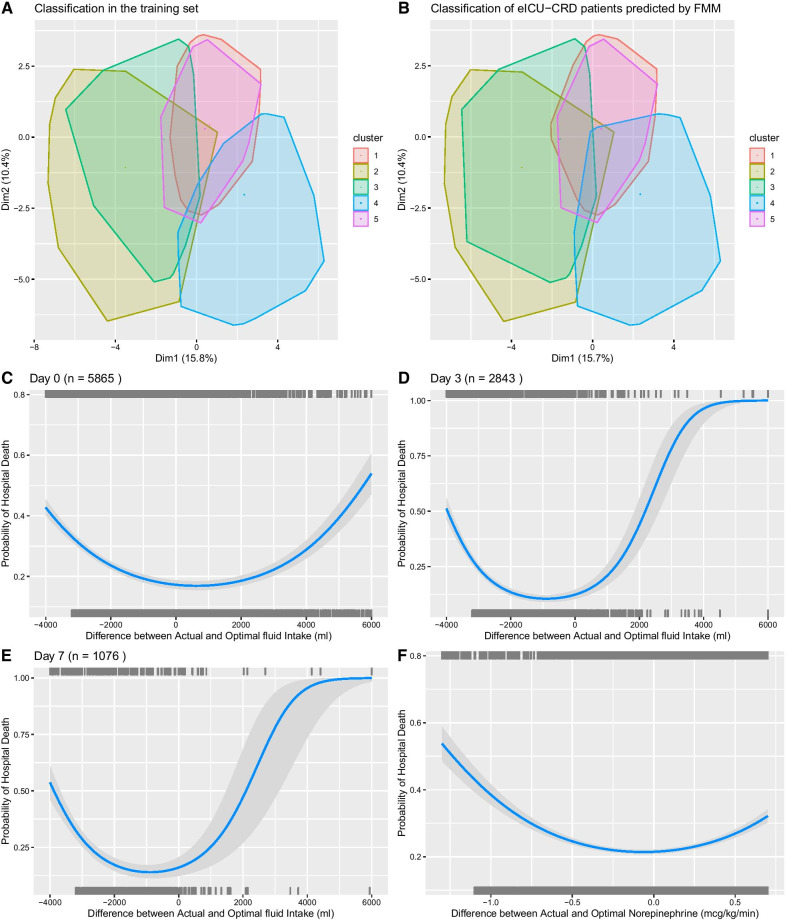
Methods: Patients with septic shock in 25 tertiary care teaching hospitals in China from January 2016 to December 2017 were enrolled in the study. Clinical and laboratory variables were collected on days 0, 1, 2, 3 and 7 after ICU admission. Subclasses of septic shock were identified by both finite mixture modeling and K-means clustering. Individualized fluid volume and norepinephrine dose were estimated using dynamic treatment regime (DTR) model to optimize the final mortality outcome. DTR models were validated in the eICU Collaborative Research Database (eICU-CRD) dataset.
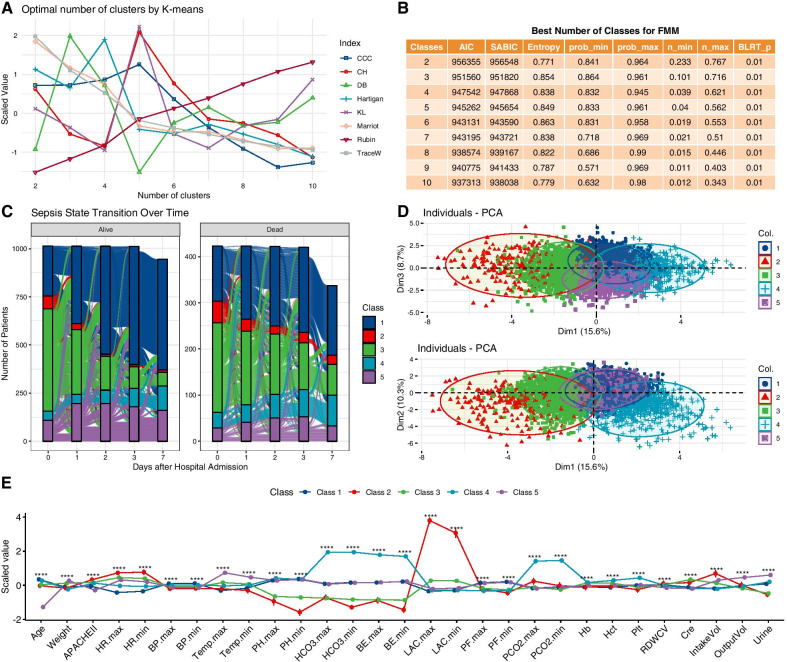
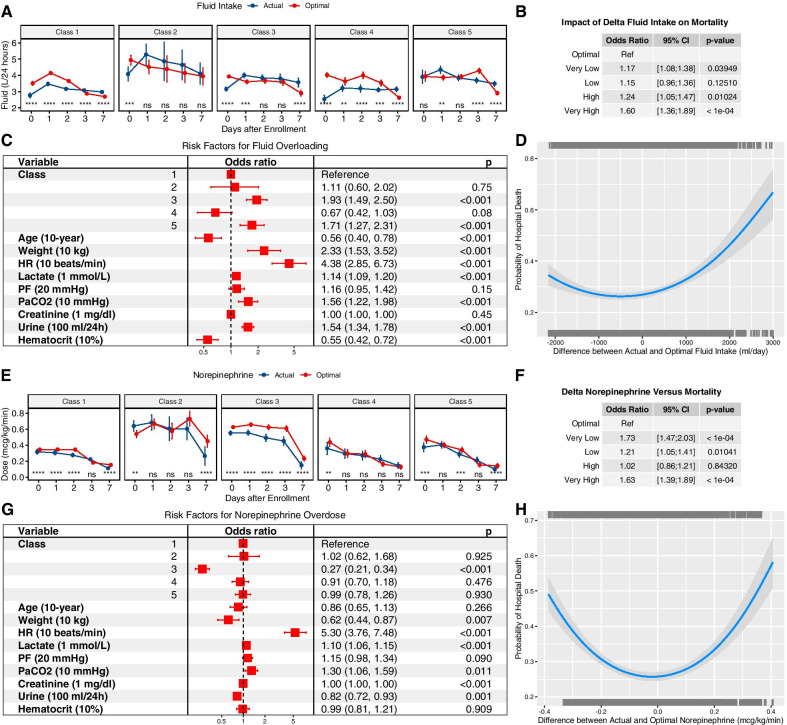
Results: A total of 1437 patients with a mortality rate of 29% were included for analysis. The finite mixture modeling and K-means clustering robustly identified five classes of septic shock. Class 1 (baseline class) accounted for the majority of patients over all days; class 2 (critical class) had the highest severity of illness; class 3 (renal dysfunction) was characterized by renal dysfunction; class 4 (respiratory failure class) was characterized by respiratory failure; and class 5 (mild class) was characterized by the lowest mortality rate (21%). The optimal fluid infusion followed the resuscitation/de-resuscitation phases with initial large volume infusion and late restricted volume infusion. While class 1 transitioned to de-resuscitation phase on day 3, class 3 transitioned on day 1. Classes 1 and 3 might benefit from early use of norepinephrine, and class 2 can benefit from delayed use of norepinephrine while waiting for adequate fluid infusion.
Conclusions: Septic shock comprises a heterogeneous population that can be robustly classified into five phenotypes. These classes can be easily identified with routine clinical variables and can help to tailor resuscitation strategy in the context of precise medicine.
Keywords: Dynamic treatment regime; Fluid resuscitation; Mortality; Sepsis.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Ospina-Tascón GA, Damiani LP, Estenssoro E, Teboul J-L, Cecconi M, Jibaja M, et al. Effect of a resuscitation strategy targeting peripheral perfusion status vs serum lactate levels on 28-day mortality among patients with septic shock: the ANDROMEDA-SHOCK Randomized Clinical Trial. JAMA Am Med Assoc. 2019;321:654–664. doi: 10.1001/jama.2019.0071. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
