Gene therapy for aromatic L-amino acid decarboxylase deficiency by MR-guided direct delivery of AAV2-AADC to midbrain dopaminergic neurons
- PMID: 34253733
- PMCID: PMC8275582
- DOI: 10.1038/s41467-021-24524-8
Gene therapy for aromatic L-amino acid decarboxylase deficiency by MR-guided direct delivery of AAV2-AADC to midbrain dopaminergic neurons
Abstract
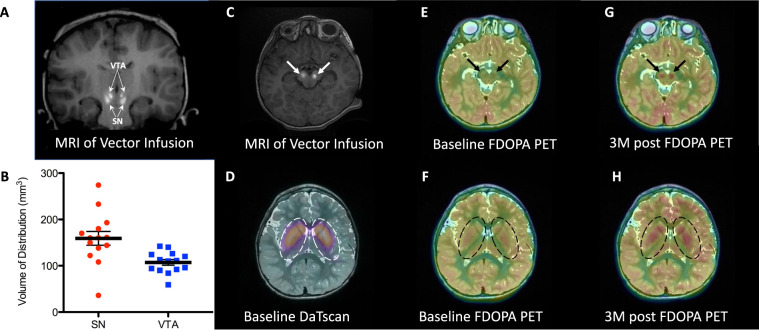
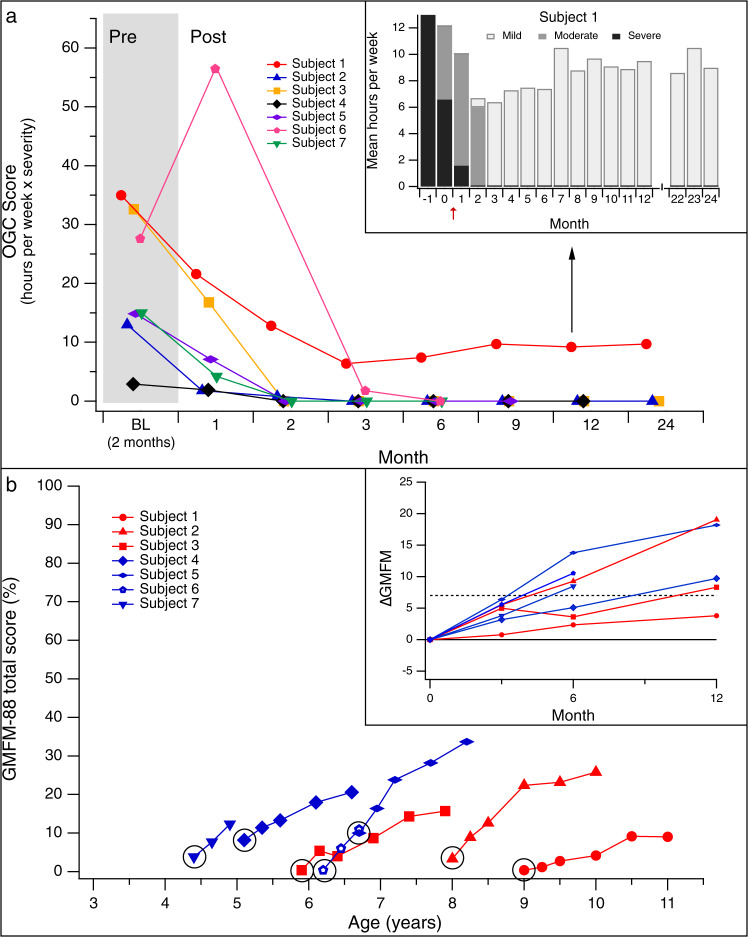
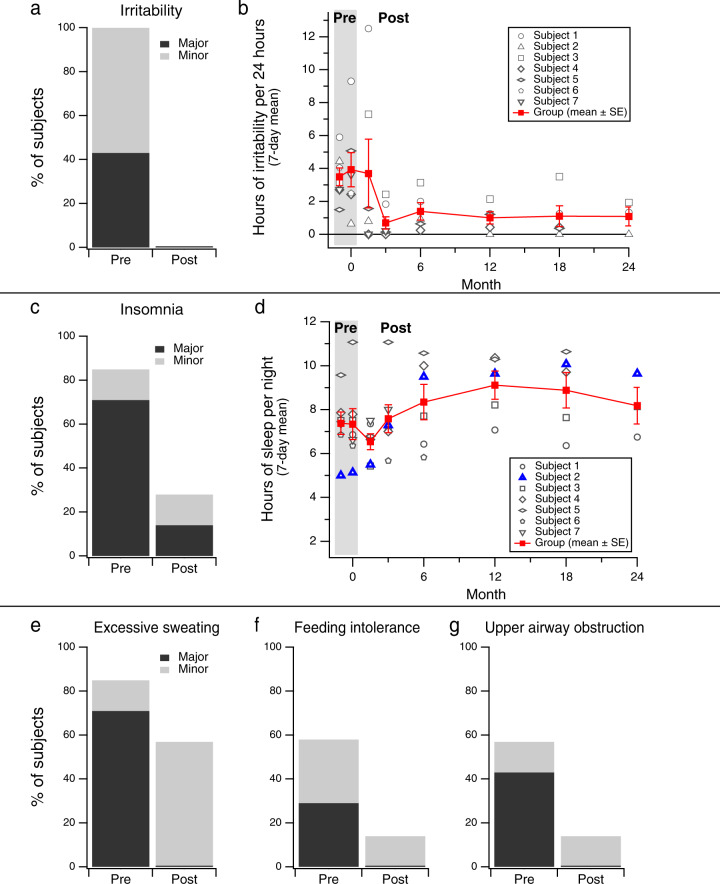
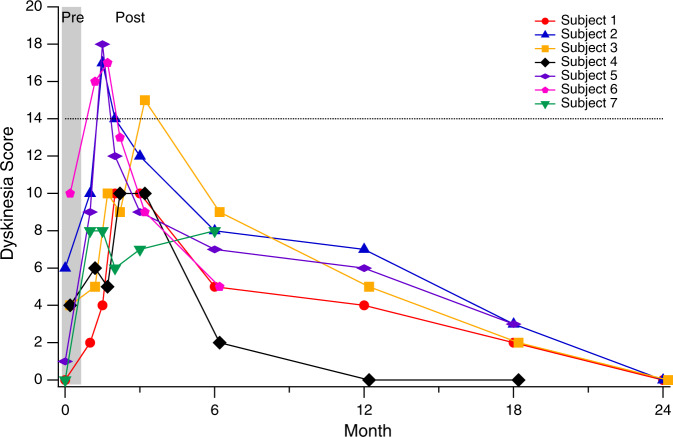
Aromatic L-amino acid decarboxylase (AADC) deficiency is a rare genetic disorder characterized by deficient synthesis of dopamine and serotonin. It presents in early infancy, and causes severe developmental disability and lifelong motor, behavioral, and autonomic symptoms including oculogyric crises (OGC), sleep disorder, and mood disturbance. We investigated the safety and efficacy of delivery of a viral vector expressing AADC (AAV2-hAADC) to the midbrain in children with AADC deficiency (ClinicalTrials.gov Identifier NCT02852213). Seven (7) children, aged 4-9 years underwent convection-enhanced delivery (CED) of AAV2-hAADC to the bilateral substantia nigra (SN) and ventral tegmental area (VTA) (total infusion volume: 80 µL per hemisphere) in 2 dose cohorts: 1.3 × 1011 vg (n = 3), and 4.2 × 1011 vg (n = 4). Primary aims were to demonstrate the safety of the procedure and document biomarker evidence of restoration of brain AADC activity. Secondary aims were to assess clinical improvement in symptoms and motor function. Direct bilateral infusion of AAV2-hAADC was safe, well-tolerated and achieved target coverage of 98% and 70% of the SN and VTA, respectively. Dopamine metabolism was increased in all subjects and FDOPA uptake was enhanced within the midbrain and the striatum. OGC resolved completely in 6 of 7 subjects by Month 3 post-surgery. Twelve (12) months after surgery, 6/7 subjects gained normal head control and 4/7 could sit independently. At 18 months, 2 subjects could walk with 2-hand support. Both the primary and secondary endpoints of the study were met. Midbrain gene delivery in children with AADC deficiency is feasible and safe, and leads to clinical improvements in symptoms and motor function.
© 2021. The Author(s).
Conflict of interest statement
N.G. reports relationships with Oscine Therapeutics (consulting) and Y-mAbs Therapeutics (consulting). K.H. reports that he is employed by Medical Neurogenetics Laboratories, a company that provides commercial diagnostic testing for aromatic
Figures