

Neurophysiological and clinical effects of the NMDA receptor antagonist lanicemine (BHV-5500) in PTSD: A randomized, double-blind, placebo-controlled trial
- PMID: 34254405
- PMCID: PMC8560553
- DOI: 10.1002/da.23194
Neurophysiological and clinical effects of the NMDA receptor antagonist lanicemine (BHV-5500) in PTSD: A randomized, double-blind, placebo-controlled trial
Abstract
Background: Posttraumatic stress disorder (PTSD) is associated with hyperarousal and stress reactivity, features consistent with behavioral sensitization. In this Phase 1b, parallel-arm, randomized, double-blind, placebo-controlled trial, we tested whether the selective low-trapping N-methyl-D-aspartate receptor (NMDAR) antagonist [Lanicemine (BHV-5500)] blocks expression of behavioral sensitization.
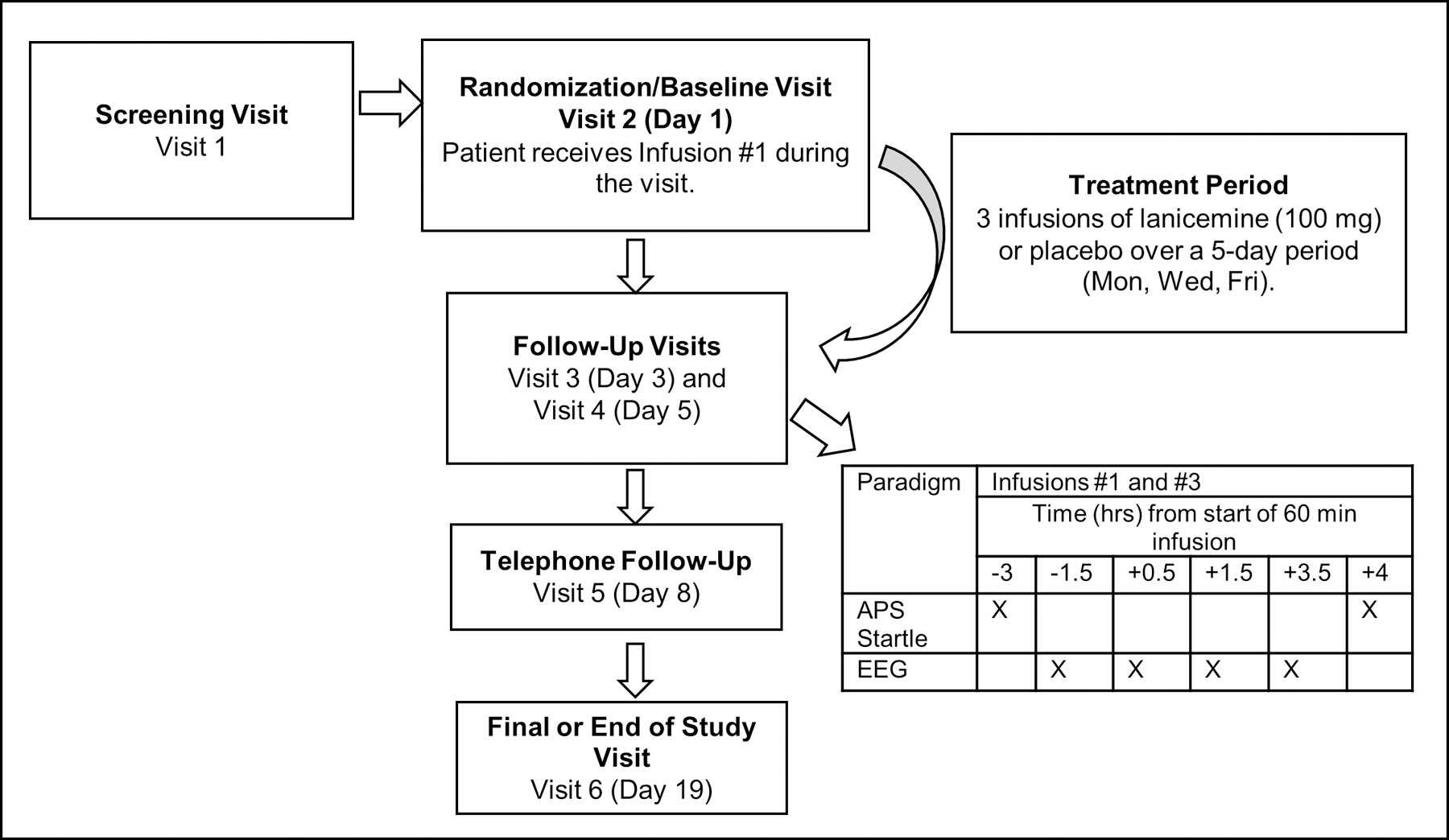
Methods: Twenty-four participants with elevated anxiety potentiated startle (APS) and moderate-to-severe PTSD symptoms received three infusions of lanicemine 1.0 mg/ml (100 mg) or matching placebo (0.9% saline) (1:1 ratio), over a 5-day period. The primary outcome was change in APS from baseline to end of third infusion. We also examined changes in EEG gamma-band oscillatory activity as measures of NMDAR target engagement and explored Clinician-Administered PTSD Scale (CAPS-5) hyperarousal scores.
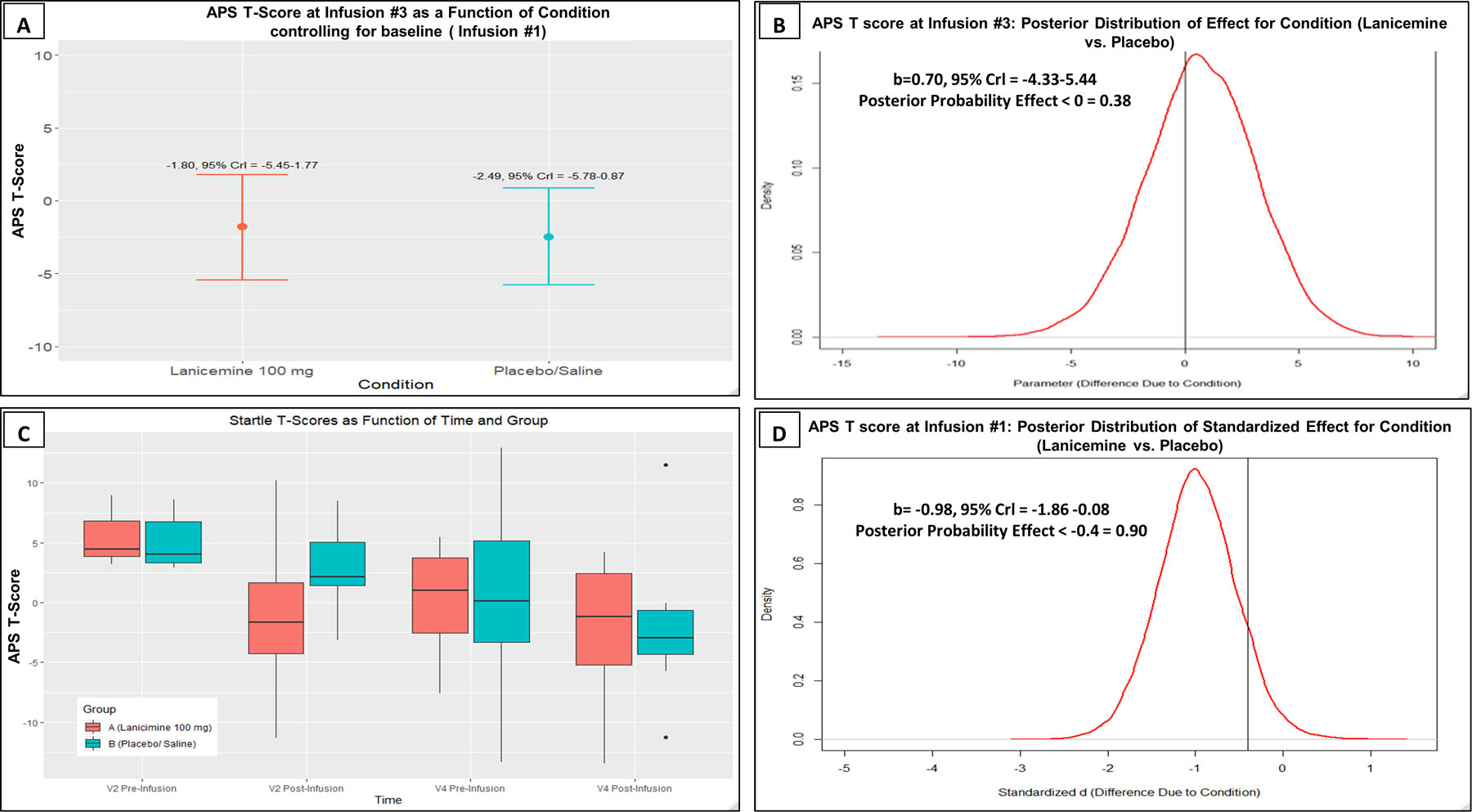
Results: Lanicemine was safe and well-tolerated with no serious adverse events. Using Bayesian statistical inference, the posterior probability that lanicemine outperformed placebo on APS T-score after three infusions was 38%. However, after the first infusion, there was a 90% chance that lanicemine outperformed placebo in attenuating APS T-score by a standardized effect size more than 0.4.
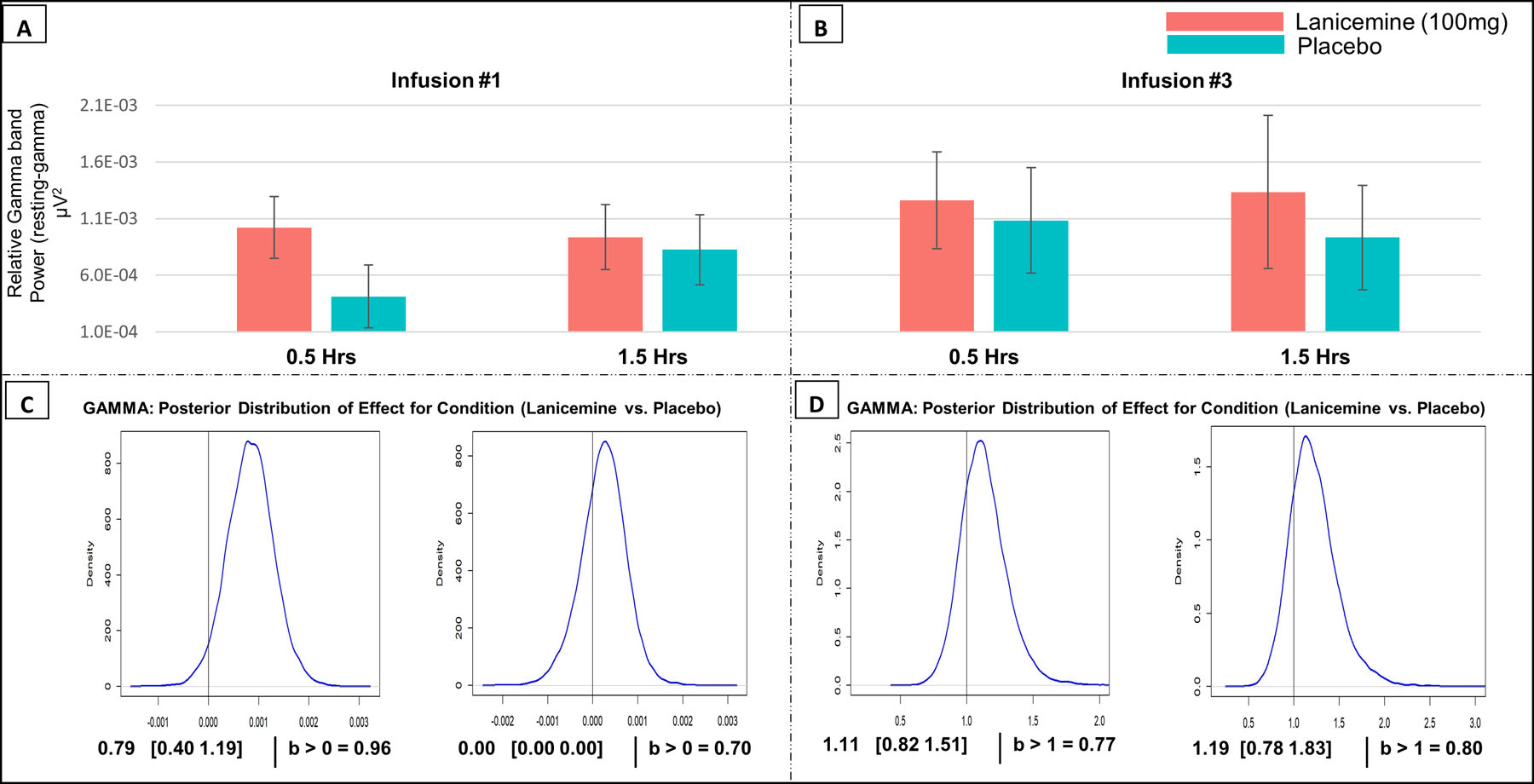
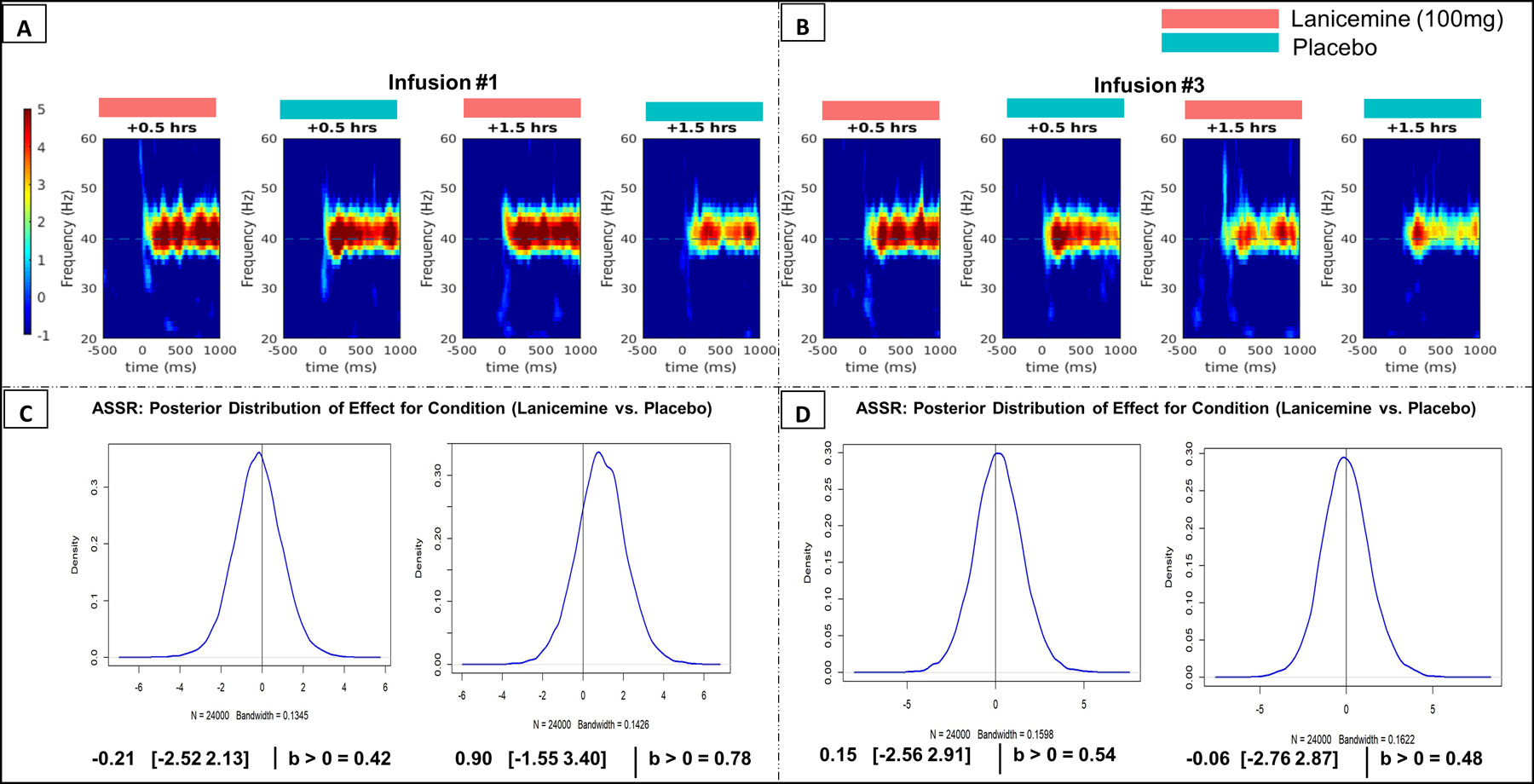
Conclusion: We demonstrated successful occupancy of lanicemine on NMDAR using gamma-band EEG and effects on hyperarousal symptoms (Cohen's d = 0.75). While lanicemine strongly attenuated APS following a single infusion, differential changes from placebo after three infusions was likely obscured by habituation effects. To our knowledge, this is the first use of APS in the context of an experimental medicine trial of a NMDAR antagonist in PTSD. These findings support selective NMDAR antagonism as a viable pharmacological strategy for salient aspects of PTSD.
Trial registration: ClinicalTrials.gov NCT03166501.
Keywords: EEG/evoked potentials; PTSD/posttraumatic stress disorder; clinical trails; pharmacotherapy; startle.
© 2021 Wiley Periodicals LLC.
Figures
References
-
- American Psychiatric Association. Diagnostic And Statistical Manual Of Mental Disorders, Fifth Edition. Arlington, VA: Am Psychiatr Publ; 2013.
-
- Stein MB, Kline NA, Matloff JL. Adjunctive olanzapine for SSRI-resistant combat-related PTSD: a double-blind, placebo-controlled study. Am J Psychiatry 2002; 159: 1777–1779. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
