

Use of Medications for Treatment of Opioid Use Disorder Among US Medicaid Enrollees in 11 States, 2014-2018
- PMID: 34255008
- PMCID: PMC8278273
- DOI: 10.1001/jama.2021.7374
Use of Medications for Treatment of Opioid Use Disorder Among US Medicaid Enrollees in 11 States, 2014-2018
Abstract
Importance: There is limited information about trends in the treatment of opioid use disorder (OUD) among Medicaid enrollees.
Objective: To examine the use of medications for OUD and potential indicators of quality of care in multiple states.
Design, setting, and participants: Exploratory serial cross-sectional study of 1 024 301 Medicaid enrollees in 11 states aged 12 through 64 years (not eligible for Medicare) with International Classification of Diseases, Ninth Revision (ICD-9 or ICD-10) codes for OUD from 2014 through 2018. Each state used generalized estimating equations to estimate associations between enrollee characteristics and outcome measure prevalence, subsequently pooled to generate global estimates using random effects meta-analyses.
Exposures: Calendar year, demographic characteristics, eligibility groups, and comorbidities.
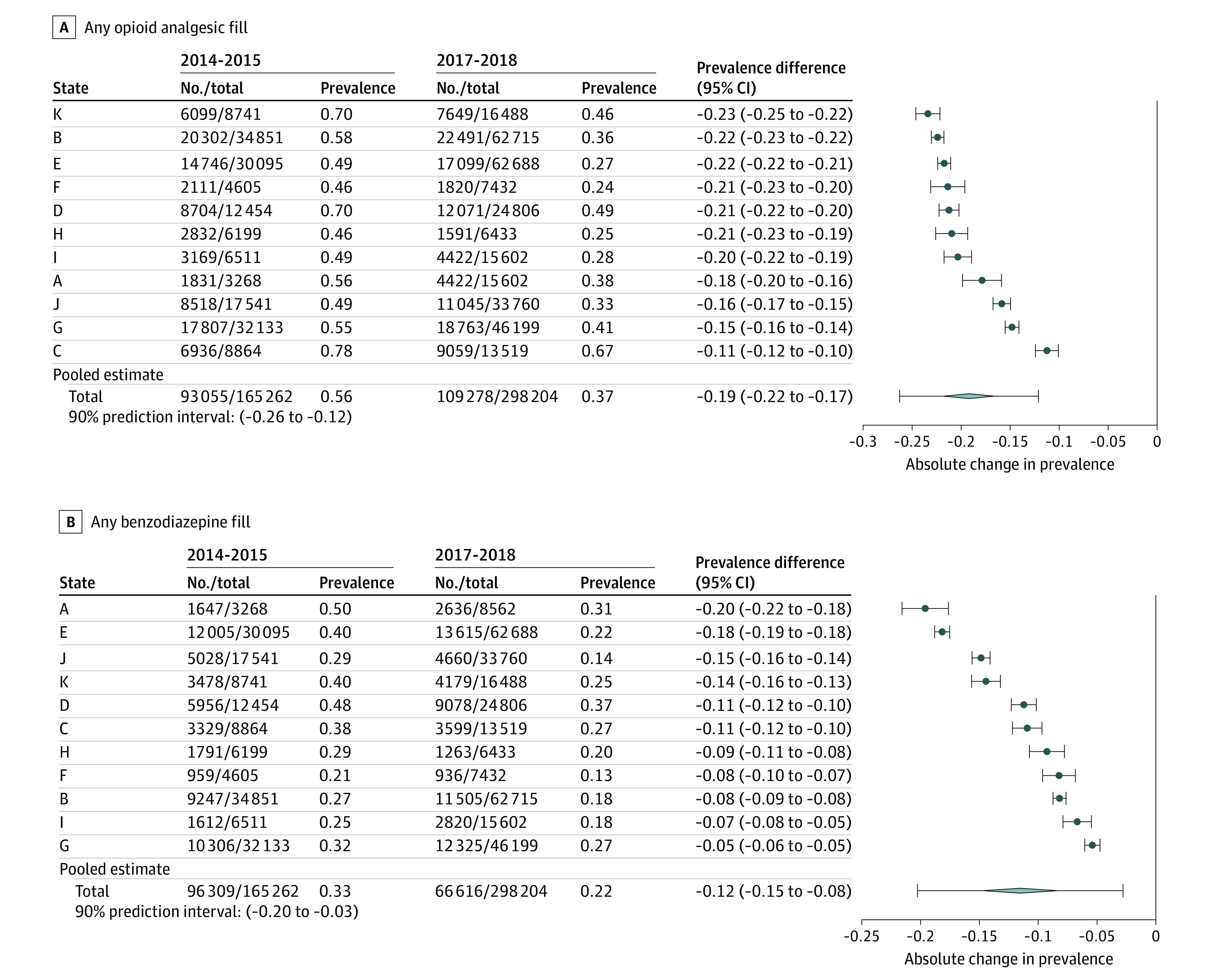
Main outcomes and measures: Use of medications for OUD (buprenorphine, methadone, or naltrexone); potential indicators of good quality (OUD medication continuity for 180 days, behavioral health counseling, urine drug tests); potential indicators of poor quality (prescribing of opioid analgesics and benzodiazepines).
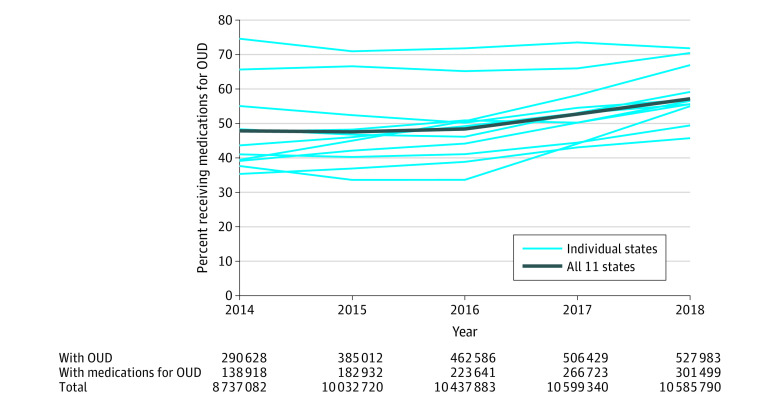
Results: In 2018, 41.7% of Medicaid enrollees with OUD were aged 21 through 34 years, 51.2% were female, 76.1% were non-Hispanic White, 50.7% were eligible through Medicaid expansion, and 50.6% had other substance use disorders. Prevalence of OUD increased in these 11 states from 3.3% (290 628 of 8 737 082) in 2014 to 5.0% (527 983 of 10 585 790) in 2018. The pooled prevalence of enrollees with OUD receiving medication treatment increased from 47.8% in 2014 (range across states, 35.3% to 74.5%) to 57.1% in 2018 (range, 45.7% to 71.7%). The overall prevalence of enrollees receiving 180 days of continuous medications for OUD did not significantly change from the 2014-2015 to 2017-2018 periods (-0.01 prevalence difference, 95% CI, -0.03 to 0.02) with state variability in trend (90% prediction interval, -0.08 to 0.06). Non-Hispanic Black enrollees had lower OUD medication use than White enrollees (prevalence ratio [PR], 0.72; 95% CI, 0.64 to 0.81; P < .001; 90% prediction interval, 0.52 to 1.00). Pregnant women had higher use of OUD medications (PR, 1.18; 95% CI, 1.11-1.25; P < .001; 90% prediction interval, 1.01-1.38) and medication continuity (PR, 1.14; 95% CI, 1.10-1.17, P < .001; 90% prediction interval, 1.06-1.22) than did other eligibility groups.
Conclusions and relevance: Among US Medicaid enrollees in 11 states, the prevalence of medication use for treatment of opioid use disorder increased from 2014 through 2018. The pattern in other states requires further research.
Conflict of interest statement
Figures



References
-
- Kaiser Family Foundation . Medicaid’s role in addressing the opioid epidemic. Published 2018. Accessed May 14, 2018. https://www.kff.org/infographic/medicaids-role-in-addressing-opioid-epid...
-
- Report to Congress: utilization management of medication-assisted treatment in Medicaid. Medicaid and CHIP Payment and Access Commission. October 2019. Accessed June 13, 2021. https://www.macpac.gov/publication/report-to-congress-utilization-manage...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
