

Review
doi: 10.1007/s00261-021-03205-6.
Epub 2021 Jul 13.
Imaging of Kaposi sarcoma
Affiliations
- PMID: 34255129
- PMCID: PMC8502139
- DOI: 10.1007/s00261-021-03205-6
Item in Clipboard
Review
Imaging of Kaposi sarcoma
Abdom Radiol (NY).
2021 Nov.
Abstract
Kaposi sarcoma (KS) is a form of cancer that primarily appears on the skin but can potentially involve internal organs. There are several types of KS. The purpose of this article is to discuss the manifestations of KS and their appearance on imaging, the differential diagnoses associated with these findings, and molecular markers associated with KS that can aid appropriate diagnosis and therapy.
Keywords: CT; HIV; Imaging; Kaposi’s sarcoma; MRI.
© 2021. The Author(s).
Conflict of interest statement
All authors declare that they have no conflict of interest.
Figures

Photograph showing solitary violaceous and dusky erythematous plaque of KS on the anterior trunk. (Picture courtesy of Dr. Neena Khanna, Professor of Dermatology, All India Institute of Medical Sciences (AIIMS), New Delhi, India)
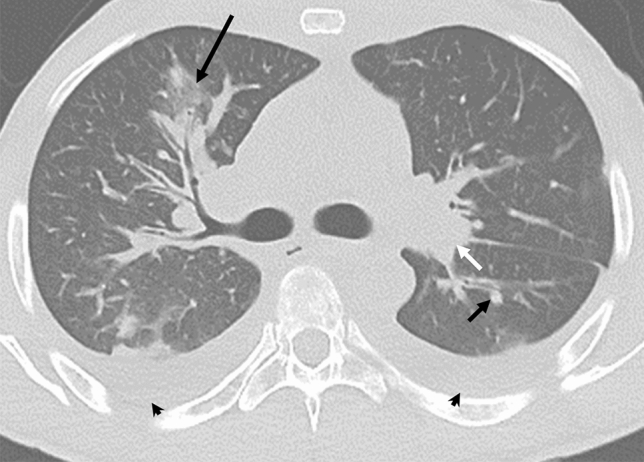
29-year-old man with KS and HIV. Axial CT showing nodular opacities (short arrow) and ground-glass halos (long arrow) surrounding the bronchovascular bundles. Lymphadenopathy (short white arrow) and bilateral pleural effusions (arrowheads) are also noted
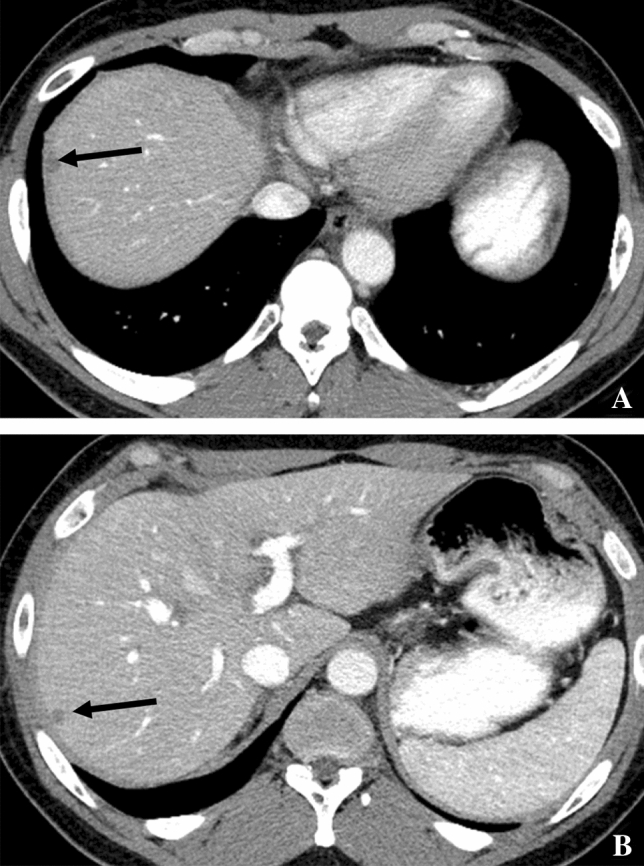
48-year-old man with KS and HIV. Contrast-enhanced axial CT A–B shows subcapsular low-attenuation lesions in the liver (arrows)
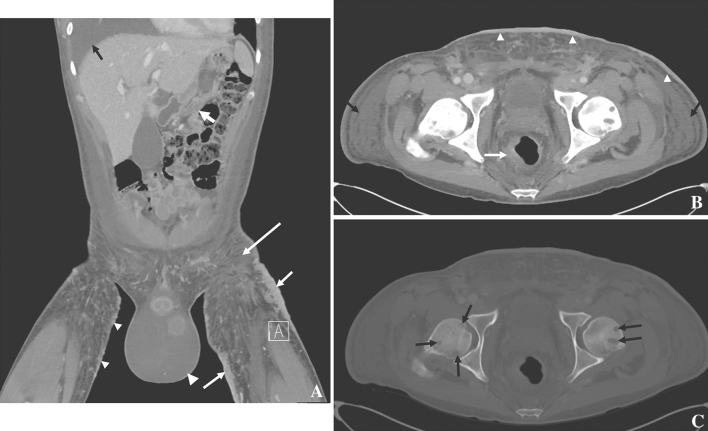
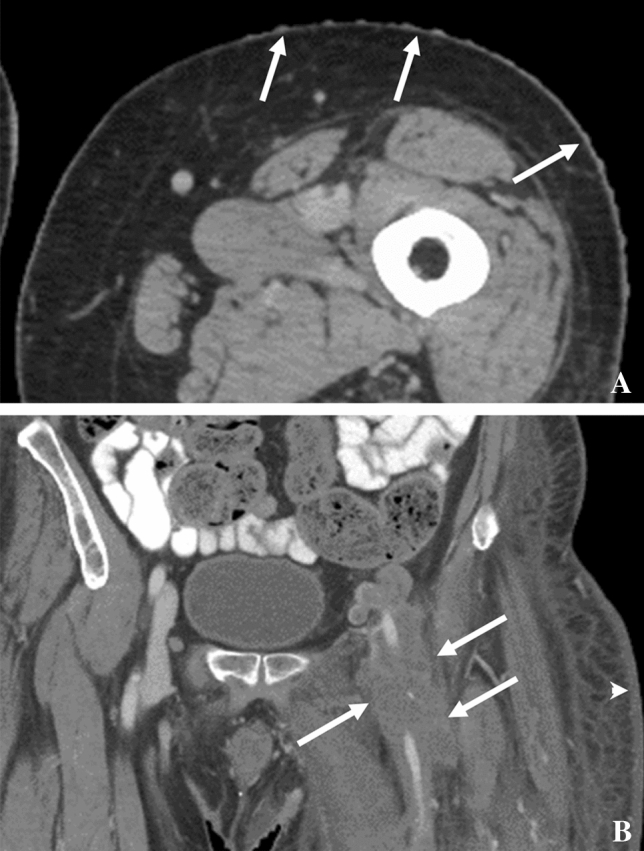
33-year-old male with HIV and KS. A Coronal contrast-enhanced CT showing antral wall thickening (fat white arrow), large and thick skin thickening (plaques, short white arrows), small skin nodules (small arrowheads), hydroceles (large arrowhead), subcutaneous edema (long arrow), and a pleural effusion (black arrow). B Axial contrast-enhanced CT showing asymmetric rectal wall thickening (white arrow), skin thickening (arrowheads), and subcutaneous edema (black arrows); C bone windows show lytic bone metastases
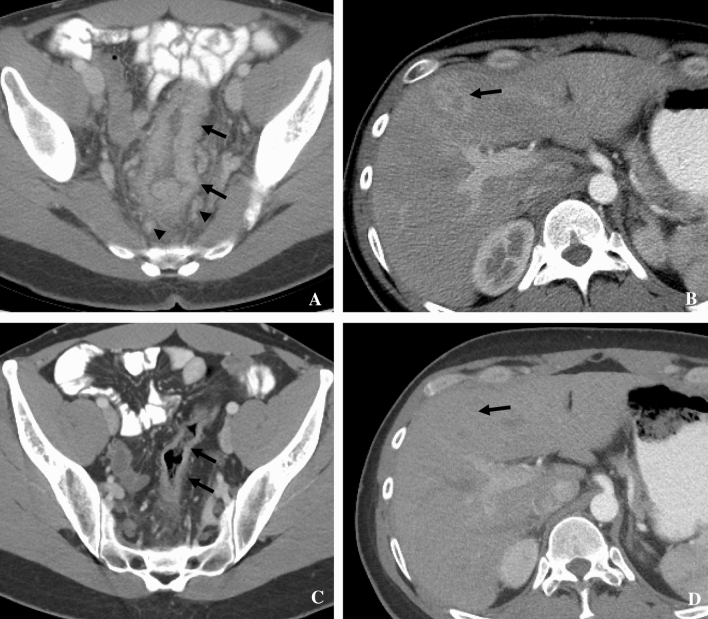
32-year-old male with HIV and KS. Contrast-enhanced CT showing A long segment thickening of the recto-sigmoid colon (arrows), enhancing perirectal lymph nodes (arrowheads), and B enhancing liver lesion secondary to KS, which resolved post-chemotherapy C, D
A A 56-year-old man with HIV and KS. Contrast-enhanced axial CT of left thigh showing nodular areas of skin thickening consistent with KS (arrows). B A 58-year-old man with HIV and KS. Contrast-enhanced coronal CT showing multiple enlarged nodes encasing the left common femoral artery (arrows) consistent with KS. Skin thickening in left gluteal region (arrowhead) is due to skin involvement by KS. Note: These images are of the same patient but from different years

52-year-old man with KS and HIV. MRI of pelvis. T2-weighted axial image showing hyperintense thickened soft tissue in glans penis (arrow)
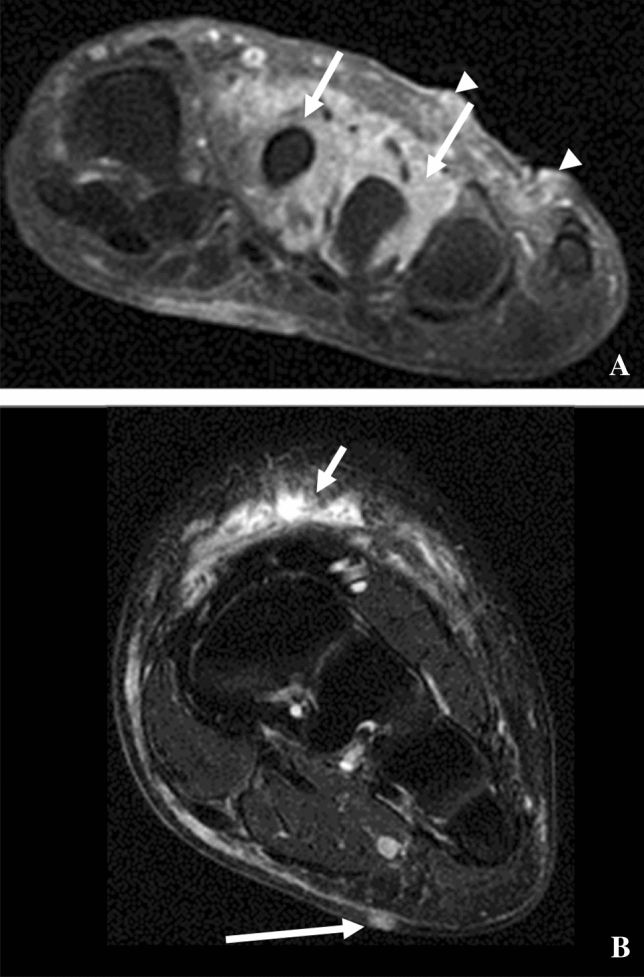
A A 67-year-old man with KS. MRI of left foot. Contrast-enhanced, fat-suppressed axial image showing thickened and enhancing soft tissue (arrows) surrounding the second and third metatarsal and enhancing skin nodules (arrowheads). B A 45-year-old man with KS. MRI lower extremity T2 fat-saturated axial image with heterogeneously hyperintense subcutaneous tissue (short arrow) and a midline plantar nodule (long arrow), both of which are consistent with KS

31-year-old male with KS and history of immunosuppression for liver transplant secondary to biliary atresia. A PET showing 18F-FDG uptake in multi-compartment lymphadenopathy (arrows). B Coronal CT showing multicompartment lymphadenopathy in the abdomen and pelvis (arrows)

KS rate per 100,000 based on the SEER 9 Areas (San Francisco, Connecticut, Detroit, Hawaii, Iowa, New Mexico, Seattle, Utah, and Atlanta) age-adjusted to the 2000 US Standard Population in relation to the HIV rate per 100,000 and the HIV/AIDS death rate per 100,000 in the USA [–62]
References
-
- Kamyab K, et al. Demographic and histopathologic study of Kaposi’s sarcoma in a dermatology clinic in the years of 2006 to 2011. Acta Med Iran. 2014;52(5):381–384. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
