

Glucagon-Like Peptide-1 Receptor Agonists and Hepatic Decompensation Events in Patients With Cirrhosis and Diabetes
- PMID: 34256144
- PMCID: PMC8743301
- DOI: 10.1016/j.cgh.2021.07.010
Glucagon-Like Peptide-1 Receptor Agonists and Hepatic Decompensation Events in Patients With Cirrhosis and Diabetes
Abstract
Background & aims: The study sought to compare the effectiveness of glucagon-like peptide-1 receptor agonists (GLP-1RAs) with dipeptidyl peptidase-4 (DPP-4) inhibitors, sulfonylureas, or sodium-glucose cotransporter-2 (SGLT-2) inhibitors in reducing decompensation events, among patients with cirrhosis and type 2 diabetes.
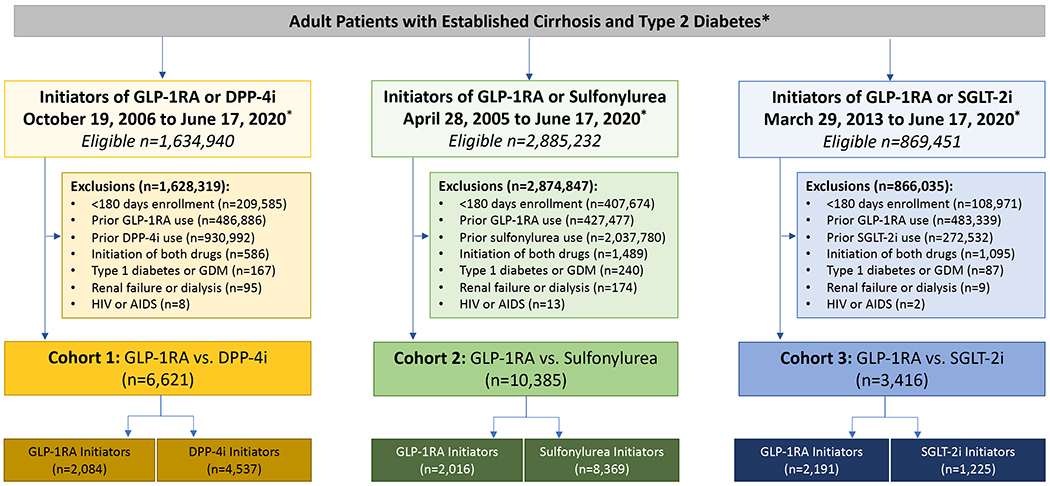
Methods: This population-based, retrospective cohort study included patients with type 2 diabetes and cirrhosis, in a commercial healthcare database (IBM MarketScan). We constructed 3 pairwise, 1:1 propensity score (PS)-matched cohorts of adults initiating GLP-1RAs or a comparator medication (ie, DPP-4 inhibitors [2006-2020], sulfonylurea [2005-2020], or SGLT-2 inhibitors [2013-2020]). Patients were followed in an as-treated approach for decompensation events (ie, ascites, spontaneous bacterial peritonitis, hepatorenal syndrome, hepatic encephalopathy, or esophageal variceal hemorrhage). Within each PS-matched cohort, we estimated hazard ratios (HRs) and 95% confidence intervals (CIs), controlling for >90 baseline characteristics.
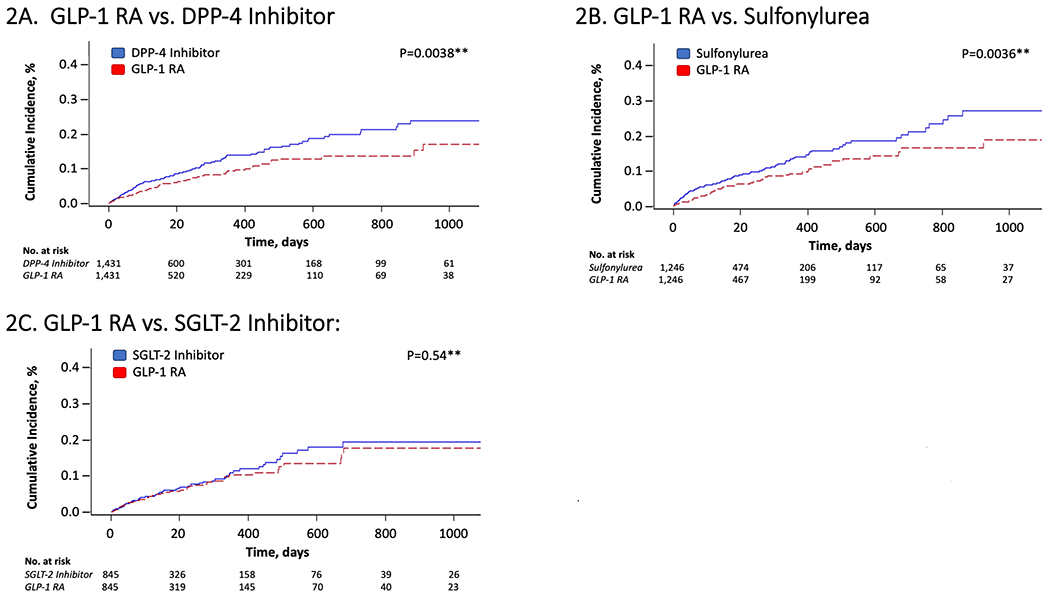
Results: Over 132 days of median follow-up (interquartile range, 73-290 days), PS-matched rates of any decompensation were significantly lower among GLP-1RA initiators, versus DPP-4 inhibitor initiators (105.2 vs 144.0 per 1000 person-years [PY]; HR, 0.68; 95% CI, 0.53-0.88; n = 1431 pairs), and versus sulfonylureas (97.3 vs 144.0 per 1000 PY; HR, 0.64; 95% CI, 0.48-0.84; n = 1246 pairs). Similar, inverse associations were found for individual decompensation events, including ascites, spontaneous bacterial peritonitis, or hepatorenal syndrome (HR, 0.66; 95% CI, 0.45-0.97; and HR, 0.66; 95% CI, 0.46-0.94, respectively); esophageal variceal hemorrhage (HR, 0.62 [95% CI, 0.41-0.92; and HR, 0.59; 95% CI, 0.37-0.92, respectively); and hepatic encephalopathy (HR, 0.76; 95% CI, 0.55-1.06; and HR, 0.60; 95% CI, 0.39-0.92, respectively). Results persisted in subgroups of patients with and without previously decompensated cirrhosis. In contrast, decompensation rates were similar when GLP-1RAs and SGLT-2 inhibitors were directly compared (103.5 vs 112.8 per 1000 PY; HR, 0.89; 95% CI, 0.62-1.28).
Conclusions: Among cirrhotic patients with type 2 diabetes, we find high rates of decompensation, consistent with previous reports; these rates were substantially lower among GLP-1RA initiators compared with DPP-4 inhibitors or sulfonylureas.
Keywords: Antidiabetic Therapy; Comparative Effectiveness; Decompensated Cirrhosis; Pharmacoepidemiology.
Copyright © 2022 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Safety and Efficacy of Glucagon-like Peptide 1 Receptor Agonists in Patients With Cirrhosis.Clin Gastroenterol Hepatol. 2022 Jun;20(6):1220-1222. doi: 10.1016/j.cgh.2021.09.023. Epub 2021 Sep 22. Clin Gastroenterol Hepatol. 2022. PMID: 34560279 No abstract available.
References
-
- Collaborators GBDCoD. Global, regional, and national age-sex specific mortality for 264 causes of death, 1980-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017;390(10100):1151–210. doi: 10.1016/S0140-6736(17)32152-9 [published Online First: 2017/09/19] - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
