

Iron overload and iron chelating agent exposure in anemia-associated outer retinal degeneration: a case report and review of the literature
- PMID: 34256738
- PMCID: PMC8278719
- DOI: 10.1186/s12886-021-02030-1
Iron overload and iron chelating agent exposure in anemia-associated outer retinal degeneration: a case report and review of the literature
Abstract
Background: Deferoxamine retinopathy is the informally designated term used to describe a characteristic pattern of outer retinal degeneration in iron-overloaded chronic anemia patients who are treated with deferoxamine. We hypothesize that insufficiently treated iron overloading and not only deferoxamine is the cause of the retinal degeneration. Our case report is based on exposure histories of two anemia patients and literature review.
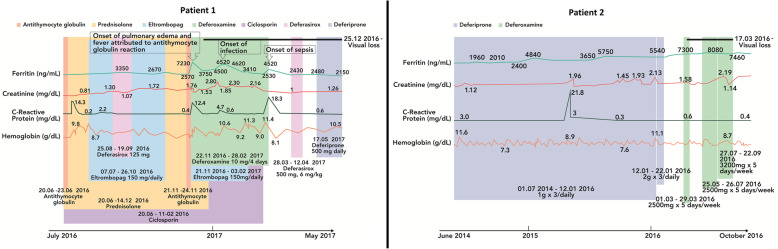
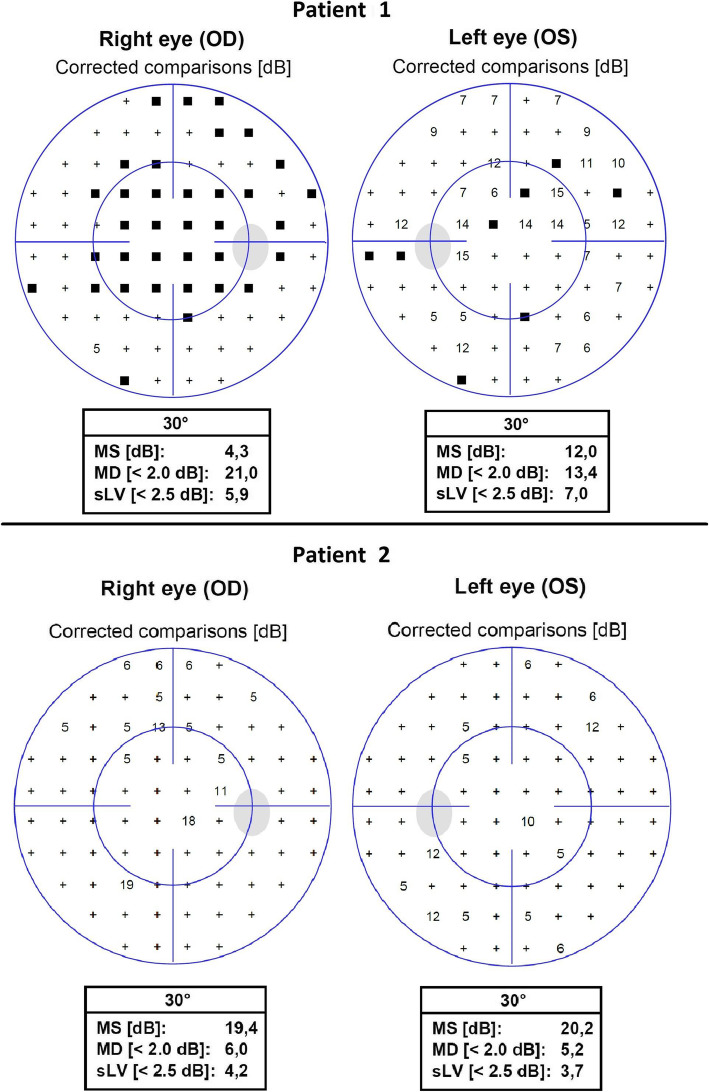
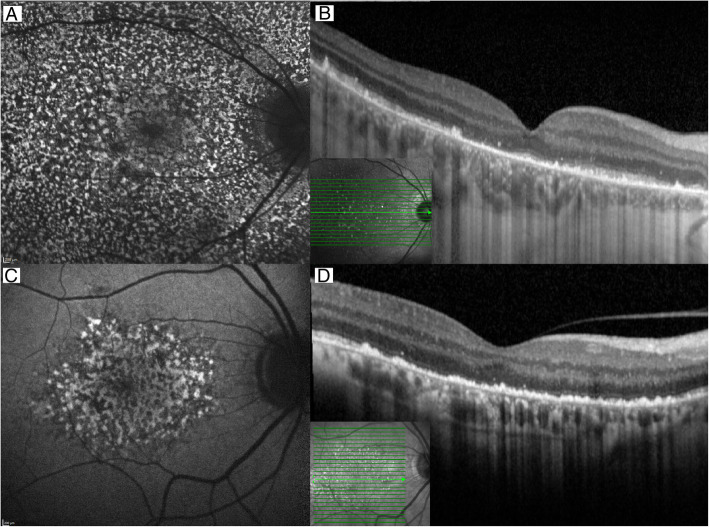
Case presentation: Both anemia patients presented with bilateral visual loss secondary to photoreceptor and retinal pigment epithelium degeneration. Chart review showed that visual loss came after a year-long slow, and rather monotonous rise in plasma ferritin concentrations, with no obvious relation to iron chelator exposure. In one patient, the onset of symptomatic visual loss came after a bout of fever followed by two additional febrile episodes, all accompanied by plasma ferritin spikes. Adjustment of iron chelation therapy did not improve visual function. Experimental studies clearly show that both systemic and intraocular exposure to iron ions can induce retinal degeneration.
Conclusion: The available evidence indicates that retinal degeneration in chronic anemia patients treated by deferoxamine is cause by insufficient iron chelation, not by deferoxamine. The actual role of iron chelating agents may be to promote a long enough survival to allow the slow development of retinal siderosis.
Keywords: Anemia; Case report; Deferoxamine; Iron chelation; Iron overload; Retinopathy.
© 2021. The Author(s).
Conflict of interest statement
ML has consulted, spoken or been a trial investigator for Novartis, Chiesi, Allergan, Bayer, Alcon, AbbVie, Biogen, Novo Nordisk, Eli Lilly, Spark Therapeutics, Nightstar, Sanofi and Roche.
Figures

References
-
- Borgna-Pignatti C, Rugolotto S, De Stefano P, et al. Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica. 2004;89(10):1187–1193. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
