

Predictability of maxillary positioning: a 3D comparison of virtual and conventional orthognathic surgery planning
- PMID: 34256775
- PMCID: PMC8276391
- DOI: 10.1186/s13005-021-00279-x
Predictability of maxillary positioning: a 3D comparison of virtual and conventional orthognathic surgery planning
Abstract
Background: Virtual surgery planning (VSP) is believed to reduce inaccuracies in maxillary positioning compared to conventional surgery planning (CSP) due to the elimination of face-bow transfer and laboratory steps. However, there is still a lack of comparative studies for the accuracy of splint-based maxillary positioning in CSP versus VSP. Therefore, the objective of this retrospective, observational study was to compare if splints produced by VSP and CSP reach postoperative outcomes within clinically acceptable limits.
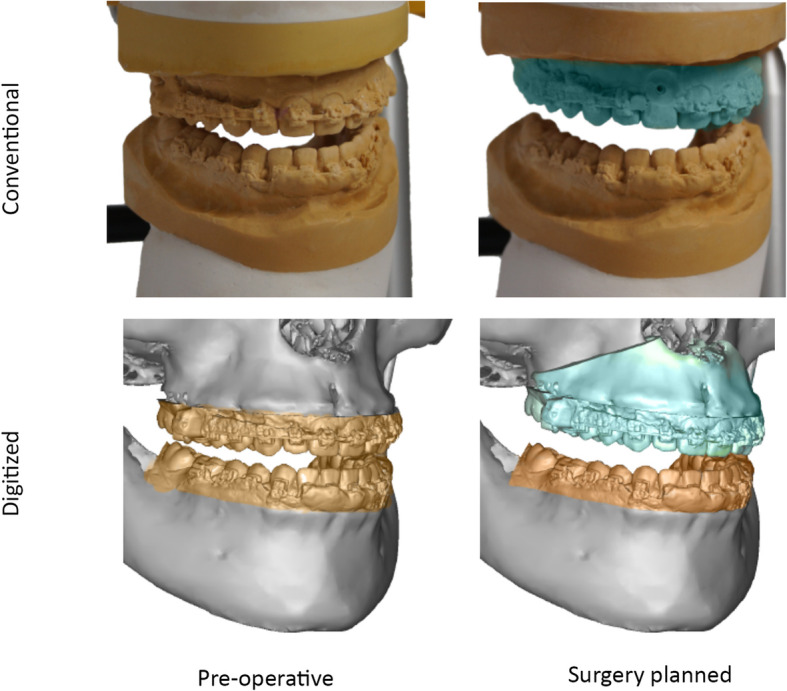
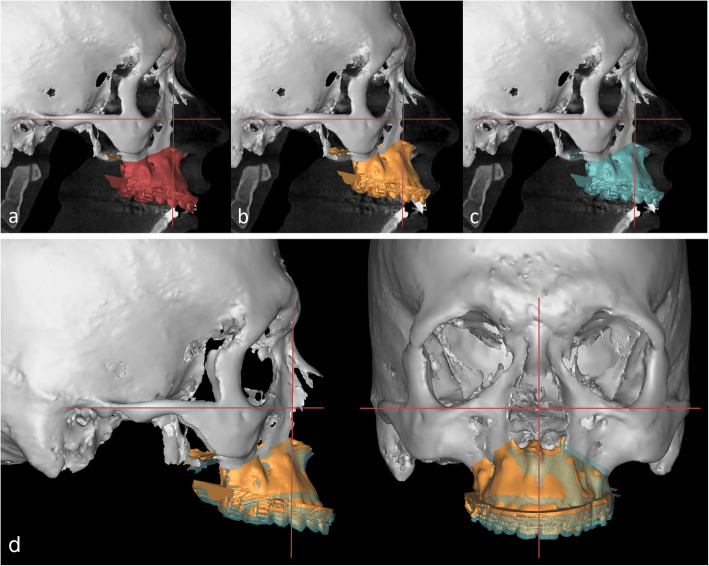
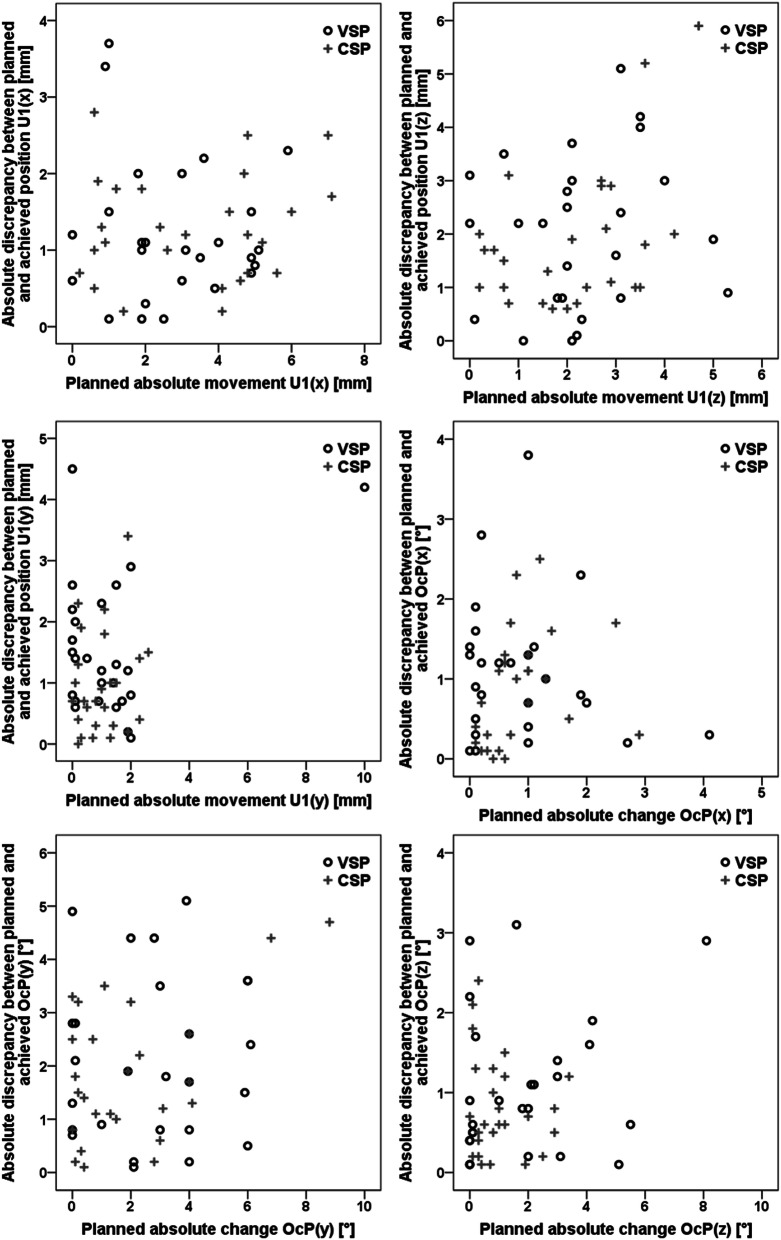
Methods: The planned and actual postoperative results of 52 patients (VSP: n = 26; CSP: n = 26) with a mean age of 24.4 ± 6.2 years were investigated by three-dimensional (3D) alignment with planning software. The conventional treatment plan was digitized, so that the evaluation of both methods was performed in the same manner using the same coordinate system. Inaccuracies were measured by sagittal, vertical and transversal deviations of the upper central incisors and the inclination of the maxillary occlusal plane between the planned and achieved maxillary positions.
Results: Both methods demonstrated significant differences between the planned and actual outcome. The highest inaccuracies were observed in vertical impaction and midline correction. No significant differences between CSP and VSP were observed in any dimension. Errors in vertical and sagittal dimension intensified each other.
Conclusions: In conclusion, splint-based surgeries reached similar results regardless of the applied planning method and splint production.
Keywords: Accuracy; BSSO; Le Fort I; Maxillary positioning; Orthodontic-surgical treatment; Orthognathic surgery; Osteotomy.
© 2021. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- Zinser MJ, Sailer HF, Ritter L, Braumann B, Maegele M, Zoller JE. A paradigm shift in orthognathic surgery? A comparison of navigation, computer-aided designed/computer-aided manufactured splints, and “classic” intermaxillary splints to surgical transfer of virtual orthognathic planning. J Oral Maxillofac Surg. 2013;71(2151):e1–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
