

Treatment resistance in psychiatry: state of the art and new directions
- PMID: 34257409
- PMCID: PMC8960394
- DOI: 10.1038/s41380-021-01200-3
Treatment resistance in psychiatry: state of the art and new directions
Abstract
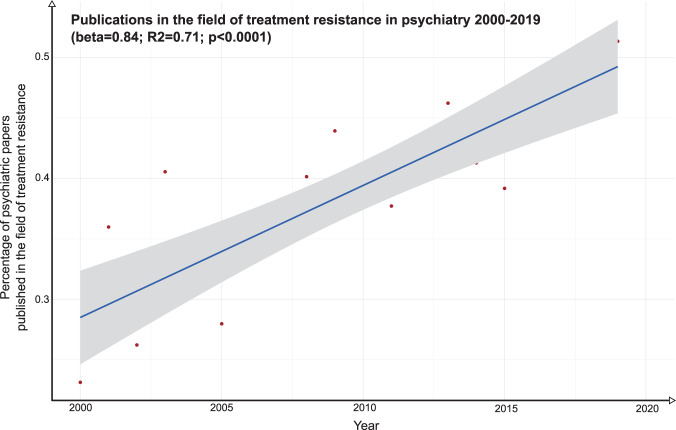
Treatment resistance affects 20-60% of patients with psychiatric disorders; and is associated with increased healthcare burden and costs up to ten-fold higher relative to patients in general. Whilst there has been a recent increase in the proportion of psychiatric research focussing on treatment resistance (R2 = 0.71, p < 0.0001), in absolute terms this is less than 1% of the total output and grossly out of proportion to its prevalence and impact. Here, we provide an overview of treatment resistance, considering its conceptualisation, assessment, epidemiology, impact, and common neurobiological models. We also review new treatments in development and future directions. We identify 23 consensus guidelines on its definition, covering schizophrenia, major depressive disorder, bipolar affective disorder, and obsessive compulsive disorder (OCD). This shows three core components to its definition, but also identifies heterogeneity and lack of criteria for a number of disorders, including panic disorder, post-traumatic stress disorder, and substance dependence. We provide a reporting check-list to aid comparisons across studies. We consider the concept of pseudo-resistance, linked to poor adherence or other factors, and provide an algorithm for the clinical assessment of treatment resistance. We identify nine drugs and a number of non-pharmacological approaches being developed for treatment resistance across schizophrenia, major depressive disorder, bipolar affective disorder, and OCD. Key outstanding issues for treatment resistance include heterogeneity and absence of consensus criteria, poor understanding of neurobiology, under-investment, and lack of treatments. We make recommendations to address these issues, including harmonisation of definitions, and research into the mechanisms and novel interventions to enable targeted and personalised therapeutic approaches.
© 2021. The Author(s).
Conflict of interest statement
Professor Howes is a part-time employee of H Lundbeck A/s and has received investigator-initiated research funding from and/or participated in advisory/ speaker meetings organised by Angellini, Autifony, Biogen, Boehringer-Ingelheim, Eli Lilly, Heptares, Global Medical Education, Invicro, Jansenn, Lundbeck, Neurocrine, Otsuka, Sunovion, Rand, Recordati, Roche and Viatris/Mylan. Neither Professor Howes nor his family have holdings or a financial stake in any pharmaceutical company. Professor Howes has a patent for the use of dopaminergic imaging. Dr Pillinger has participated in speaker meetings organised by Lundbeck, Otsuka, Sunovion, Schwabe Pharma and Recordati. Professor Thase has served as an adviser or consultant for Acadia, Akili, Alkermes, Allergan (Forest, Naurex), Boehringer-Ingelheim, Calla, Cerecor, Clexio Biosciences, Fabre-Kramer Pharmaceuticals, Gerson Lehrman Group, Guidepoint Global, H. Lundbeck A/S, Jazz Pharmaceuticals, Janssen (Johnson & Johnson), Moksha8 Pharmaceuticals, Nestle, Neuralstem, Novartis International AG, Otsuka Pharmaceutical Company, Perception Neuroscience, Pfizer, Sage Therapeutics, Seelos Therapeutics, Sunovion Pharmaceuticals, and Takeda; he has received grant support from Acadia, the Agency for Healthcare Research and Quality, Alkermes, Allergan (Forest, Naurex), AssureRx Health, Avanir, Axsome Therapeutics, Intracellular, Janssen Pharmaceutica (Johnson & Johnson), Myriad (Assurex), NIMH, Otsuka Pharmaceutical Company, the Patient Centered Outcomes Research Institute, and Takeda; and he has received royalties from American Psychiatric Press, Inc., Guilford Publications, Herald House, and W.W. Norton & Company. His spouse is a Vice President of Open Health (formerly Peloton Advantage), which does business with a number of pharmaceutical companies.
Figures

Comment in
-
Autoimmune obsessive-compulsive disorder with novel anti-CNS autoantibodies in cerebrospinal fluid.Mol Psychiatry. 2022 Oct;27(10):3926-3928. doi: 10.1038/s41380-022-01688-3. Epub 2022 Jul 13. Mol Psychiatry. 2022. PMID: 35831487 Free PMC article. No abstract available.
-
Cautious optimism regarding the use of home-based neuromodulation to treat depression.Lancet Psychiatry. 2023 Mar;10(3):156-157. doi: 10.1016/S2215-0366(23)00028-7. Epub 2023 Jan 29. Lancet Psychiatry. 2023. PMID: 36724797 No abstract available.
