

Prognostic stratification for IDH-wild-type lower-grade astrocytoma by Sanger sequencing and copy-number alteration analysis with MLPA
- PMID: 34257410
- PMCID: PMC8277860
- DOI: 10.1038/s41598-021-93937-8
Prognostic stratification for IDH-wild-type lower-grade astrocytoma by Sanger sequencing and copy-number alteration analysis with MLPA
Abstract
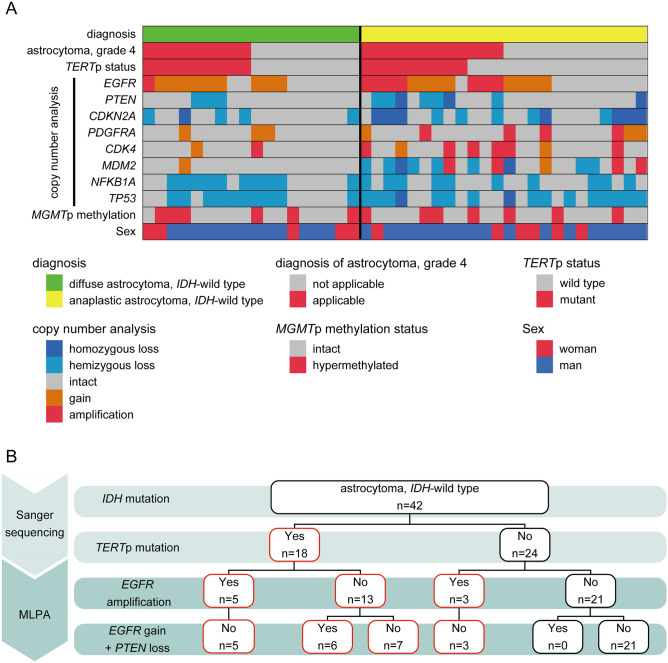
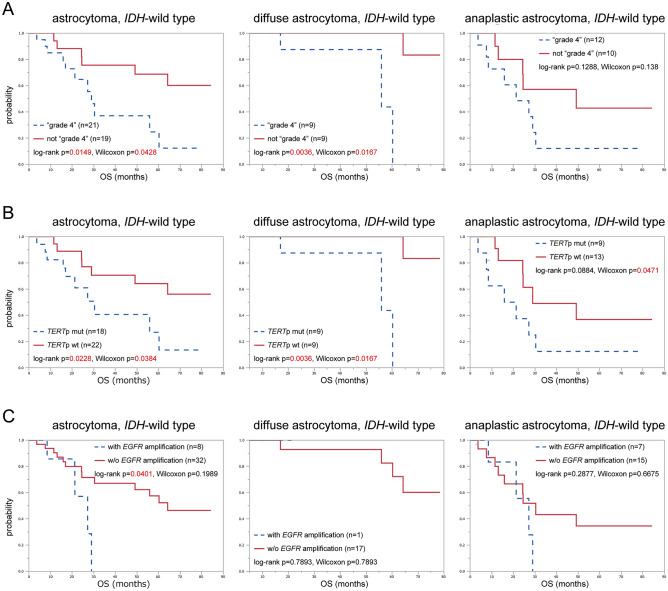
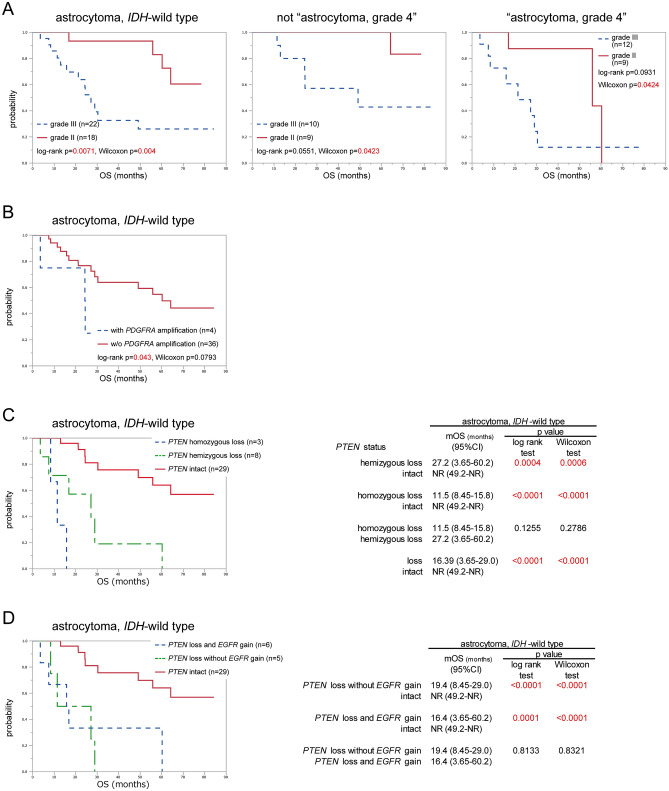
The characteristics of IDH-wild-type lower-grade astrocytoma remain unclear. According to cIMPACT-NOW update 3, IDH-wild-type astrocytomas with any of the following factors show poor prognosis: combination of chromosome 7 gain and 10 loss (+ 7/- 10), and/or EGFR amplification, and/or TERT promoter (TERTp) mutation. Multiplex ligation-dependent probe amplification (MLPA) can detect copy number alterations at reasonable cost. The purpose of this study was to identify a precise, cost-effective method for stratifying the prognosis of IDH-wild-type astrocytoma. Sanger sequencing, MLPA, and quantitative methylation-specific PCR were performed for 42 IDH-wild-type lower-grade astrocytomas surgically treated at Kyoto University Hospital, and overall survival was analysed for 40 patients who underwent first surgery. Of the 42 IDH-wild-type astrocytomas, 21 were classified as grade 4 using cIMPACT-NOW update 3 criteria and all had either TERTp mutation or EGFR amplification. Kaplan-Meier analysis confirmed the prognostic significance of cIMPACT-NOW criteria, and World Health Organization grade was also prognostic. Cox regression hazard model identified independent significant prognostic indicators of PTEN loss (risk ratio, 9.75; p < 0.001) and PDGFRA amplification (risk ratio, 13.9; p = 0.002). The classification recommended by cIMPACT-NOW update 3 could be completed using Sanger sequencing and MLPA. Survival analysis revealed PTEN and PDGFRA were significant prognostic factors for IDH-wild-type lower-grade astrocytoma.
© 2021. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
TERT promoter mutation status is necessary and sufficient to diagnose IDH-wildtype diffuse astrocytic glioma with molecular features of glioblastoma.Acta Neuropathol. 2021 Aug;142(2):323-338. doi: 10.1007/s00401-021-02337-9. Epub 2021 Jun 20. Acta Neuropathol. 2021. PMID: 34148105
-
IDH mutant lower grade (WHO Grades II/III) astrocytomas can be stratified for risk by CDKN2A, CDK4 and PDGFRA copy number alterations.Brain Pathol. 2020 May;30(3):541-553. doi: 10.1111/bpa.12801. Epub 2019 Dec 3. Brain Pathol. 2020. PMID: 31733156 Free PMC article.
-
Use of telomerase promoter mutations to mark specific molecular subsets with reciprocal clinical behavior in IDH mutant and IDH wild-type diffuse gliomas.J Neurosurg. 2018 Apr;128(4):1102-1114. doi: 10.3171/2016.11.JNS16973. Epub 2017 Jun 16. J Neurosurg. 2018. PMID: 28621624
-
Grading of adult diffuse gliomas according to the 2021 WHO Classification of Tumors of the Central Nervous System.Lab Invest. 2022 Feb;102(2):126-133. doi: 10.1038/s41374-021-00667-6. Epub 2021 Sep 9. Lab Invest. 2022. PMID: 34504304 Review.
-
Diffuse astrocytic glioma, IDH-Wildtype, with molecular features of glioblastoma, WHO grade IV: A single-institution case series and review.J Neurooncol. 2021 Mar;152(1):89-98. doi: 10.1007/s11060-020-03677-4. Epub 2021 Jan 3. J Neurooncol. 2021. PMID: 33389563 Review.
Cited by
-
Unraveling the heterogeneity of WHO grade 4 gliomas: insights from clinical, imaging, and molecular characterization.Discov Oncol. 2025 Feb 3;16(1):111. doi: 10.1007/s12672-025-01811-0. Discov Oncol. 2025. PMID: 39899184 Free PMC article.
-
Clinical and imaging characteristics of supratentorial glioma with IDH2 mutation.Neuroradiology. 2024 Jun;66(6):973-981. doi: 10.1007/s00234-024-03361-8. Epub 2024 Apr 24. Neuroradiology. 2024. PMID: 38653782
-
IDH wild-type lower-grade gliomas with glioblastoma molecular features: a systematic review and meta-analysis.Brain Tumor Pathol. 2023 Jul;40(3):143-157. doi: 10.1007/s10014-023-00463-8. Epub 2023 May 22. Brain Tumor Pathol. 2023. PMID: 37212969
-
RANO 2.0: critical updates and practical considerations for radiological assessment in neuro-oncology.Jpn J Radiol. 2025 Jun 30. doi: 10.1007/s11604-025-01821-6. Online ahead of print. Jpn J Radiol. 2025. PMID: 40586994 Review.
-
Correlation between brain functional connectivity and neurocognitive function in patients with left frontal glioma.Sci Rep. 2022 Nov 8;12(1):18302. doi: 10.1038/s41598-022-22493-6. Sci Rep. 2022. PMID: 36347905 Free PMC article.
References
-
- Cavenee WK, Louis DN, Ohgaki H, Wiestler OD, International Agency for Research on Cancer . WHO Classification of Tumours of the Central Nervous System. 4. International Agency for Research on Cancer; 2016.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
