

Landscape of Biomarkers in Non-small Cell Lung Cancer Using Comprehensive Genomic Profiling and PD-L1 Immunohistochemistry
- PMID: 34257540
- PMCID: PMC8262230
- DOI: 10.3389/pore.2021.592997
Landscape of Biomarkers in Non-small Cell Lung Cancer Using Comprehensive Genomic Profiling and PD-L1 Immunohistochemistry
Abstract
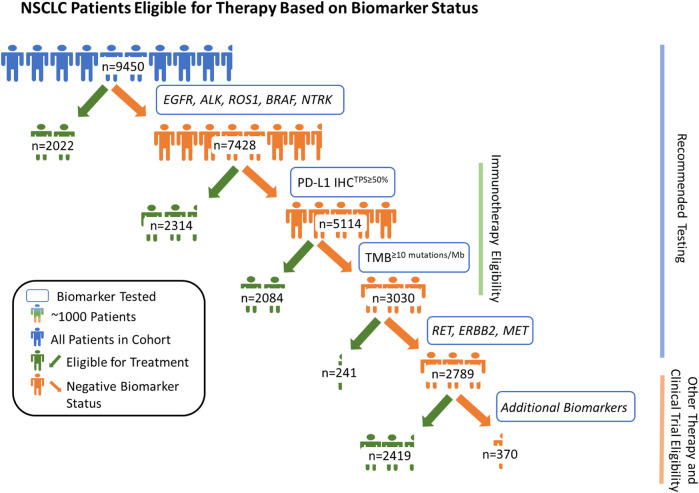
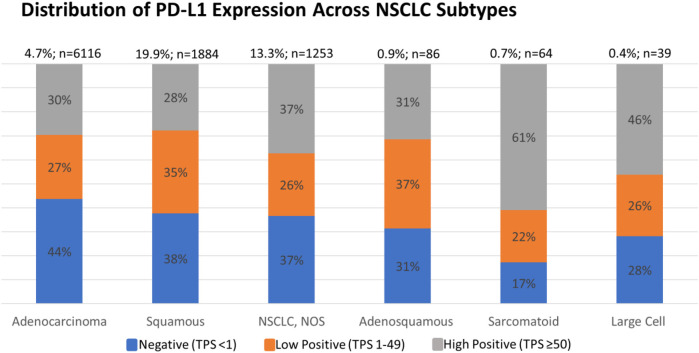
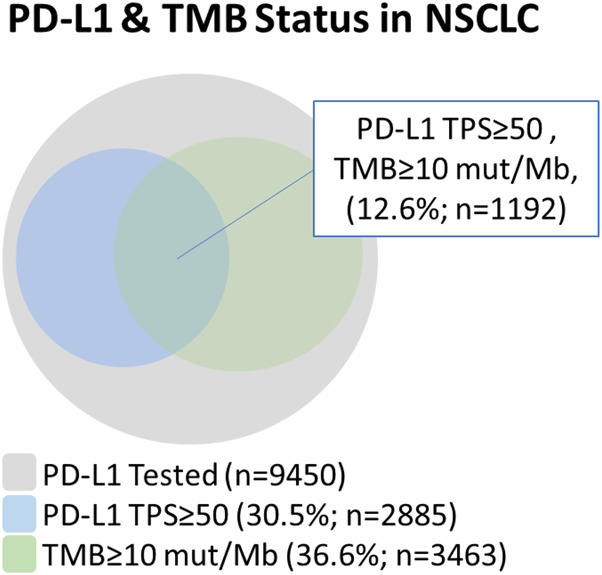
Comprehensive genomic profiling (CGP) and immunohistochemistry (IHC) are important biomarker tools used for patients with non-small cell lung cancer (NSCLC) given the expanding number of standard-of-care therapies that require companion diagnostic testing. We examined 9450 NSCLC real-world patient samples that underwent both CGP and programmed death-ligand 1 (PD-L1) IHC to understand the biomarker landscape in this patient cohort. By assessing National Comprehensive Cancer Network (NCCN)-recommended biomarkers including genomic alterations, tumor mutational burden (≥10 mutations/Mb cut-off), and PD-L1 expression (Tumor Proportion Score (TPS) ≥ 50% cut-off), we show that CGP + PD-L1 IHC yielded potentially actionable results for 70.5% of the 9,450 patients with NSCLC. Among the remaining 29.5% (2,789/9,450) of patients, 86.7% (2,419/2,789) were potentially eligible for another biomarker-associated therapy and/or clinical trial based on their genomic profile. In addition, in the PD-L1TPS≥50% disease subset, BRAF mutations, MET mutations, MET amplifications, and KRAS mutations were significantly enriched; and in the PD-L1TPS<50%, EGFR mutations, ERBB2 mutations, STK11 mutations, and KEAP1 mutations were enriched. These findings highlight the improved clinical utility of combining CGP with IHC to expand the biomarker-guided therapeutic options available for patients with NSCLC, relative to single biomarker testing alone.
Keywords: PD-L1; biomarkers; comprehensive genomic profiling; immunohistochemistry; non-small cell lung cancer.
Copyright © 2021 Huang, Severson, Haberberger, Duncan, Hemmerich, Edgerly, Ferguson, Frampton, Owens, Williams, Elvin, Vergilio, Killian, Lin, Morley, McEwan, Holmes, Danziger, Cohen, Sathyan, McGregor, Reddy, Venstrom, Anhorn, Alexander, Brown, Ross and Ramkissoon.
Conflict of interest statement
Authors RH, ES, JH, DD, AH, CE, NF, CO, CB, JR, SR, GF, EW, JE, JV, JK, DL, SM, DM, OH, ND, PS, KM, PR, JV, RA, and BA were employed by the company Foundation Medicine, Inc., which is a wholly subsidiary of Roche and receive stock from Roche. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Society AC. Cancer Facts and figures. Atlanta, GA: American Cancer Society Inc. (2019).
-
- FaD Administration. List of cleared or approved companion diagnostic devices (in vitro and imaging tools). White Oak, MD: FaD Administration; (2019).
-
- NCCN, NCCN Clinical practice guidelines in Oncology, non-small cell lung cancer. Version 5. Plymouth Meeting, PA; NCCN; (2019).
-
- Eberhard DA, Johnson BE, Amler LC, Goddard AD, Heldens SL, Herbst RS, et al. Mutations in the epidermal growth factor receptor and in KRAS are predictive and prognostic indicators in patients with non-small-cell lung cancer treated with chemotherapy alone and in combination with erlotinib. J Clin Oncol (2005) 23(25), 5900–9. 10.1200/JCO.2005.02.857 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous