

Development and Validation of a Multivariable Predictive Model for Mortality of COVID-19 Patients Demanding High Oxygen Flow at Admission to ICU: AIDA Score
- PMID: 34257816
- PMCID: PMC8245230
- DOI: 10.1155/2021/6654388
Development and Validation of a Multivariable Predictive Model for Mortality of COVID-19 Patients Demanding High Oxygen Flow at Admission to ICU: AIDA Score
Abstract
Introduction: Risk stratification is an important aspect of COVID-19 management, especially in patients admitted to ICU as it can provide more useful consumption of health resources, as well as prioritize critical care services in situations of overwhelming number of patients.
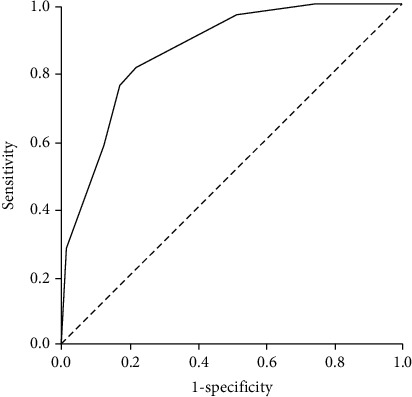
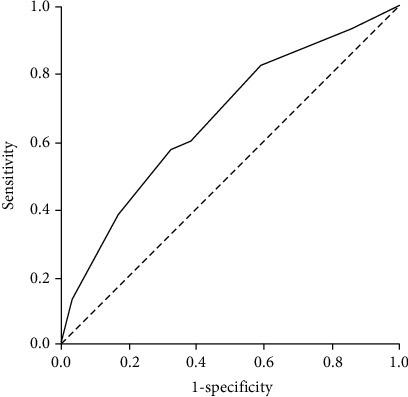
Materials and methods: A multivariable predictive model for mortality was developed using data solely from a derivation cohort of 160 COVID-19 patients with moderate to severe ARDS admitted to ICU. The regression coefficients from the final multivariate model of the derivation study were used to assign points for the risk model, consisted of all significant variables from the multivariate analysis and age as a known risk factor for COVID-19 patient mortality. The newly developed AIDA score was arrived at by assigning 5 points for serum albumin and 1 point for IL-6, D dimer, and age. The score was further validated on a cohort of 304 patients admitted to ICU due to the severe form of COVID-19.
Results: The study population included 160 COVID-19 patients admitted to ICU in the derivation and 304 in the validation cohort. The mean patient age was 66.7 years (range, 20-93 years), with 68.1% men and 31.9% women. Most patients (76.8%) had comorbidities with hypertension (67.7%), diabetes (31.7), and coronary artery disease (19.3) as the most frequent. A total of 316 patients (68.3%) were treated with mechanical ventilation. Ninety-six (60.0%) in the derivation cohort and 221 (72.7%) patients in the validation cohort had a lethal outcome. The population was divided into the following risk categories for mortality based on the risk model score: low risk (score 0-1) and at-risk (score > 1). In addition, patients were considered at high risk with a risk score > 2. By applying the risk model to the validation cohort (n = 304), the positive predictive value was 78.8% (95% CI 75.5% to 81.8%); the negative predictive value was 46.6% (95% CI 37.3% to 56.2%); the sensitivity was 82.4% (95% CI 76.7% to 87.1%), and the specificity was 41.0% (95% CI 30.3% to 52.3%). The C statistic was 0.863 (95% CI 0.805-0.921) and 0.665 (95% CI 0.598-0.732) in the derivation and validation cohorts, respectively, indicating a high discriminative value of the proposed score.
Conclusion: In the present study, AIDA score showed a valuable significance in estimating the mortality risk in patients with the severe form of COVID-19 disease at admission to ICU. Further external validation on a larger group of patients is needed to provide more insights into the utility of this score in everyday practice.
Copyright © 2021 Marija Zdravkovic et al.
Conflict of interest statement
The authors declare that there is no conflict of interest regarding the publication of this paper.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
