

Refracture and mortality following hospitalization for severe osteoporotic fractures: The Fractos Study
- PMID: 34258503
- PMCID: PMC8260818
- DOI: 10.1002/jbm4.10507
Refracture and mortality following hospitalization for severe osteoporotic fractures: The Fractos Study
Abstract
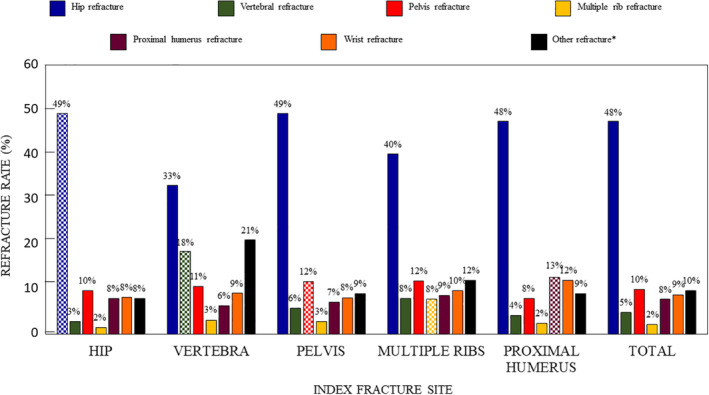
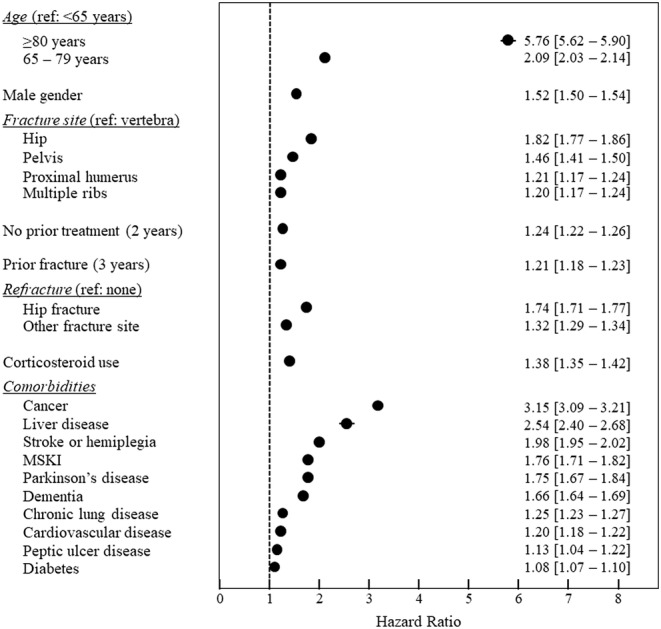
Severe osteoporotic fractures (hip, proximal humerus, pelvic, vertebral and multiple rib fractures) carry an increased risk of mortality. This retrospective cohort study in the French national healthcare database aimed to estimate refracture and mortality rates after severe osteoporotic fractures at different sites, and to identify mortality-related variables. A total of 356,895 patients hospitalized for severe osteoporotic fracture between 2009 and 2014 inclusive were analyzed. The cohort was followed for 2 to 8 years up to the study end or until the patient died. Data were extracted on subsequent hospitalizations, refracture events, treatments, comorbidities of interest and survival. Time to refracture and survival were described using Kaplan-Meier analysis by site of fracture and overall. Mortality risk factors were identified using a Cox model. Hip fractures accounted for 60.4% of the sample (N = 215,672). In the 12 months following fracture, 58,220 patients (16.7%) received a specific osteoporosis treatment, of whom 21,228 were previously treatment-naïve. The 12-month refracture rate was 6.3% (95% confidence interval [CI], 6.2%-6.3%), ranging from 4.0% (95% CI, 3.7%-4.3%) for multiple rib fractures to 7.8% (95% CI, 7.5%-8.1%) for pelvic fractures. Twelve-month all-cause mortality was 12.8% (95% CI, 12.7%-12.9%), ranging from 5.0% (95% CI, 4.7%-5.2%) for vertebral fractures to 16.6% (95% CI, 16.4%-16.7%) for hip fractures. Osteoporosis-related mortality risk factors included fracture site, previous osteoporotic fracture (hazard ratio 1.21; 95% CI, 1.18-1.23), hip refracture (1.74; 95% CI, 1.71-1.77), and no prior osteoporosis treatment (1.24; 95% CI, 1.22-1.26). Comorbid cancer (3.15; 95% CI, 3.09-3.21) and liver disease (2.54; 95% CI, 2.40-2.68) were also strongly associated with mortality. In conclusion, severe osteoporotic fractures, including certain non-hip nonvertebral fractures, carry a high burden in terms of mortality and refracture risk. However, most patients received no anti-osteoporotic treatment. The findings emphasize the importance of better management of patients with severe fractures, and of developing effective strategies to reduce fracture risk in patients with osteoporosis. © 2021 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
Keywords: FRACTURE PREVENTION; FRACTURE RISK ASSESSMENT; GENERAL POPULATION STUDIES; OSTEOPOROSIS; THERAPEUTICS.
© 2021 The Authors. JBMR Plus published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research.
Figures
References
-
- Al‐Sari UA, Tobias J, Clark E. Health‐related quality of life in older people with osteoporotic vertebral fractures: a systematic review and meta‐analysis. Osteoporos Int. 2016;27(10):2891‐2900. - PubMed
-
- Martin AR, Sornay‐Rendu E, Chandler JM, Duboeuf F, Girman CJ, Delmas PD. The impact of osteoporosis on quality‐of‐life: the OFELY cohort. Bone. 2002;31(1):32‐36. - PubMed
-
- Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low‐trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009;301(5):513‐521. - PubMed
-
- Briggs AM, Sun W, Miller LJ, Geelhoed E, Huska A, Inderjeeth CA. Hospitalisations, admission costs and re‐fracture risk related to osteoporosis in Western Australia are substantial: a 10‐year review. Aust N Z J Public Health. 2015;39(6):557‐562. - PubMed
LinkOut - more resources
Full Text Sources