

Factors associated with antihypertensive treatment intensification and deintensification in older outpatients
- PMID: 34258575
- PMCID: PMC8254109
- DOI: 10.1016/j.ijchy.2021.100098
Factors associated with antihypertensive treatment intensification and deintensification in older outpatients
Abstract
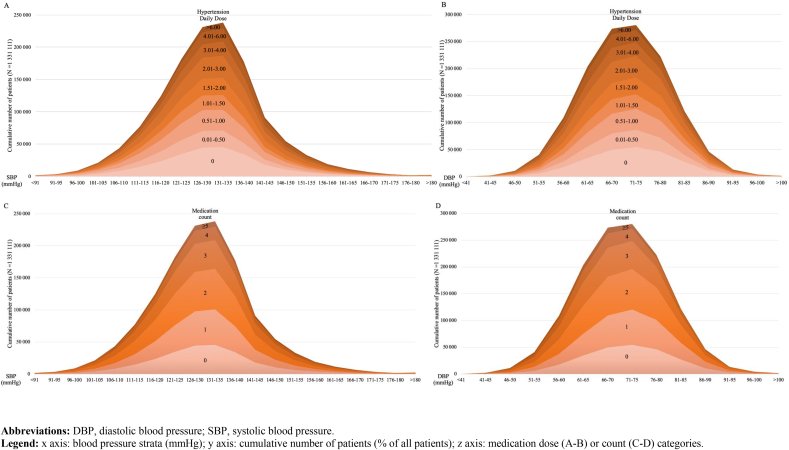
Background: New hypertension performance measures encourage more intensive treatment in older adults. Treatment intensification includes starting new medications and increasing the dose of old ones. Medication dose is particularly important to older adults, given their vulnerability to dose-related side effects. We previously validated a standardized measure of beneficial doses tested in hypertension trials, Hypertension Daily Dose (HDD).
Aim of the study: To test whether changes in treatment intensity using HDD was associated with systolic blood pressure (SBP) and patient characteristics.
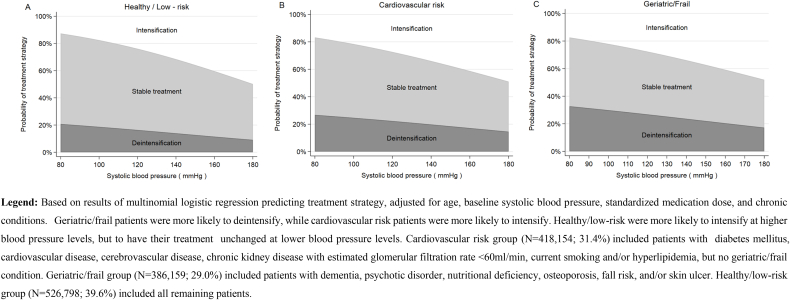
Methods: Longitudinal study of all Veterans aged ≥65 years with a diagnosis of hypertension. We defined 3 groups of risk: 1) cardiovascular risk; 2) geriatric/frail; 3) low-risk (comparator). Using multinomial regression, we assessed the probability of deintensification, intensification, vs. stable treatment, according to SBP and group.
Results: Among 1,331,111 Veterans, 19.9% had deintensification, and 29.6% intensification. Deintensification decreased, while intensification increased, with SBP. Compared to low-risk patients, cardiovascular risk patients had 1.11 (95% CI 1.10-1.13) times the odds of intensifying, and geriatric/frail patients 1.45 (95%CI 1.43-1.47) times the odds of deintensifying.
Discussion: Patient-level HDD change was consistent with an expected association with cardiovascular risk and geriatric/frail conditions, suggesting that HDD can be used longitudinally to assess hypertension treatment modification in large health systems.
Keywords: Deintensification; Elderly; Hypertension; Intensification; Medication; Patterns; Treatment; Veterans.
© 2021 The Authors.
Figures
Similar articles
-
Clinical outcomes of modifying hypertension treatment intensity in older adults treated to low blood pressure.J Am Geriatr Soc. 2021 Oct;69(10):2831-2841. doi: 10.1111/jgs.17295. Epub 2021 Jun 7. J Am Geriatr Soc. 2021. PMID: 34097300 Free PMC article.
-
A Cross-Sectional Study of Overtreatment and Deintensification of Antidiabetic and Antihypertensive Medications in Diabetes Mellitus: The TEMD Overtreatment Study.Diabetes Ther. 2020 May;11(5):1045-1059. doi: 10.1007/s13300-020-00779-0. Epub 2020 Feb 22. Diabetes Ther. 2020. PMID: 32088879 Free PMC article.
-
Adding a New Medication Versus Maximizing Dose to Intensify Hypertension Treatment in Older Adults : A Retrospective Observational Study.Ann Intern Med. 2021 Dec;174(12):1666-1673. doi: 10.7326/M21-1456. Epub 2021 Oct 5. Ann Intern Med. 2021. PMID: 34606315 Free PMC article.
-
Deprescribing in Older Nursing Home Patients: Focus on Innovative Composite Measures for Dosage Deintensification.Innov Aging. 2017 Dec 20;1(2):igx031. doi: 10.1093/geroni/igx031. eCollection 2017 Sep. Innov Aging. 2017. PMID: 30564752 Free PMC article. Review.
-
Hypertension Management in Older and Frail Older Patients.Circ Res. 2019 Mar 29;124(7):1045-1060. doi: 10.1161/CIRCRESAHA.118.313236. Circ Res. 2019. PMID: 30920928 Review.
Cited by
-
Therapeutic patient education and treatment intensification of diabetes and hypertension in subjects with newly diagnosed type 2 diabetes mellitus: a longitudinal study.Endocrine. 2024 Oct;86(1):127-134. doi: 10.1007/s12020-024-03839-8. Epub 2024 Apr 24. Endocrine. 2024. PMID: 38656749
References
-
- Onder G., van der Cammen T.J., Petrovic M., Somers A., Rajkumar C. Strategies to reduce the risk of iatrogenic illness in complex older adults. Age Ageing. 2013;42:284–291. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
