

Accelerating precision medicine in metastatic prostate cancer
- PMID: 34258585
- PMCID: PMC8274325
- DOI: 10.1038/s43018-020-00141-0
Accelerating precision medicine in metastatic prostate cancer
Abstract
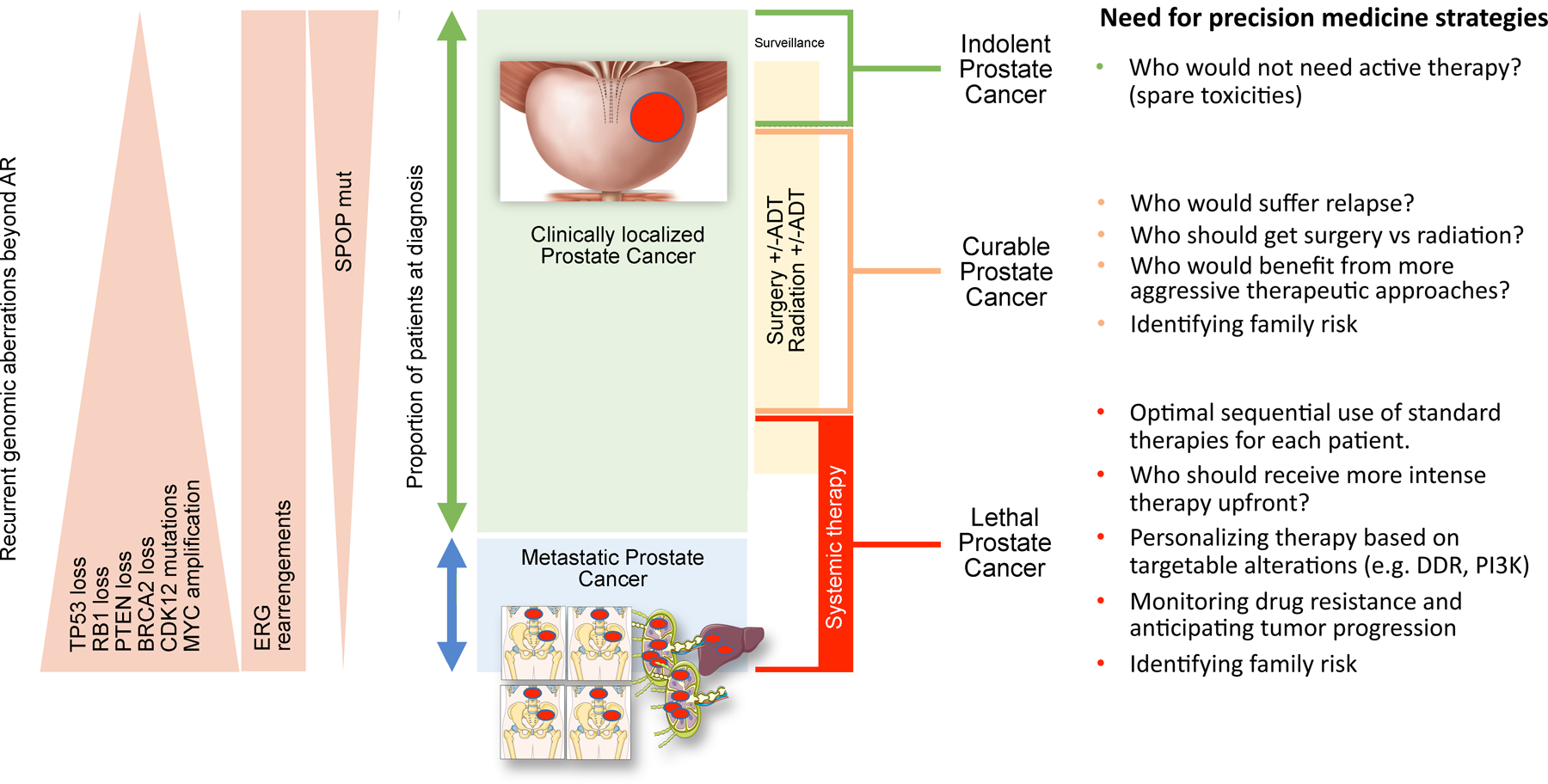
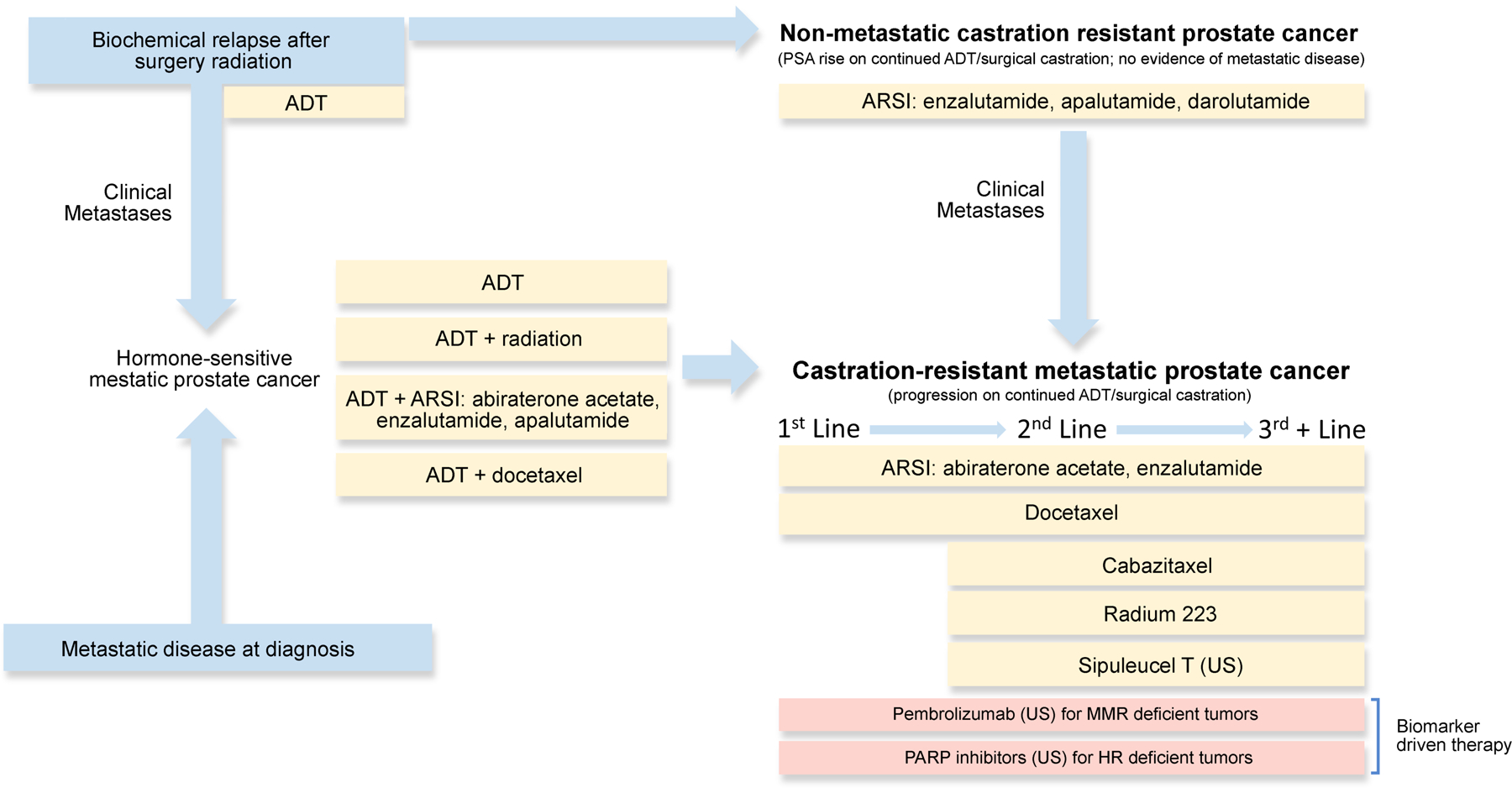
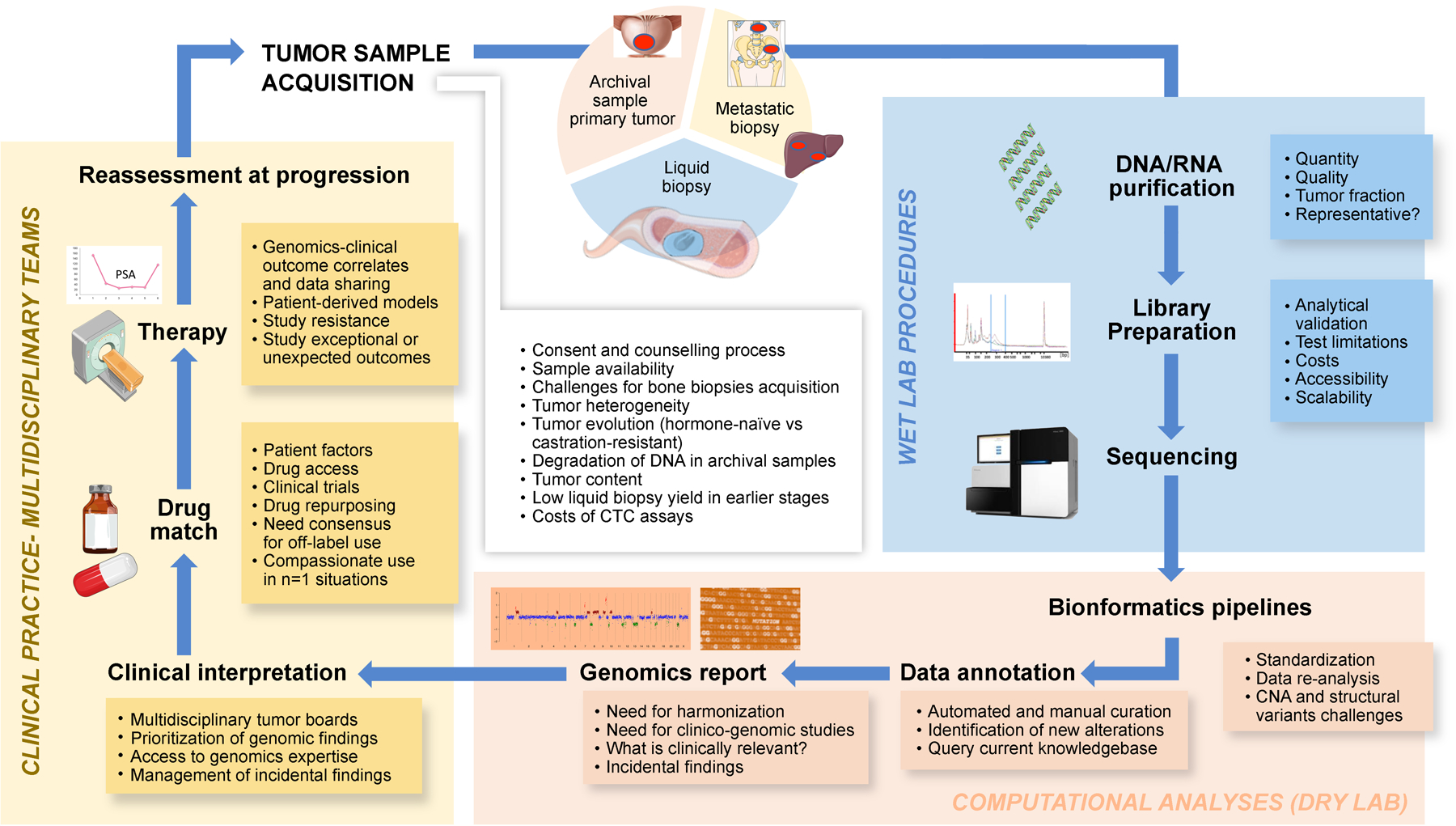
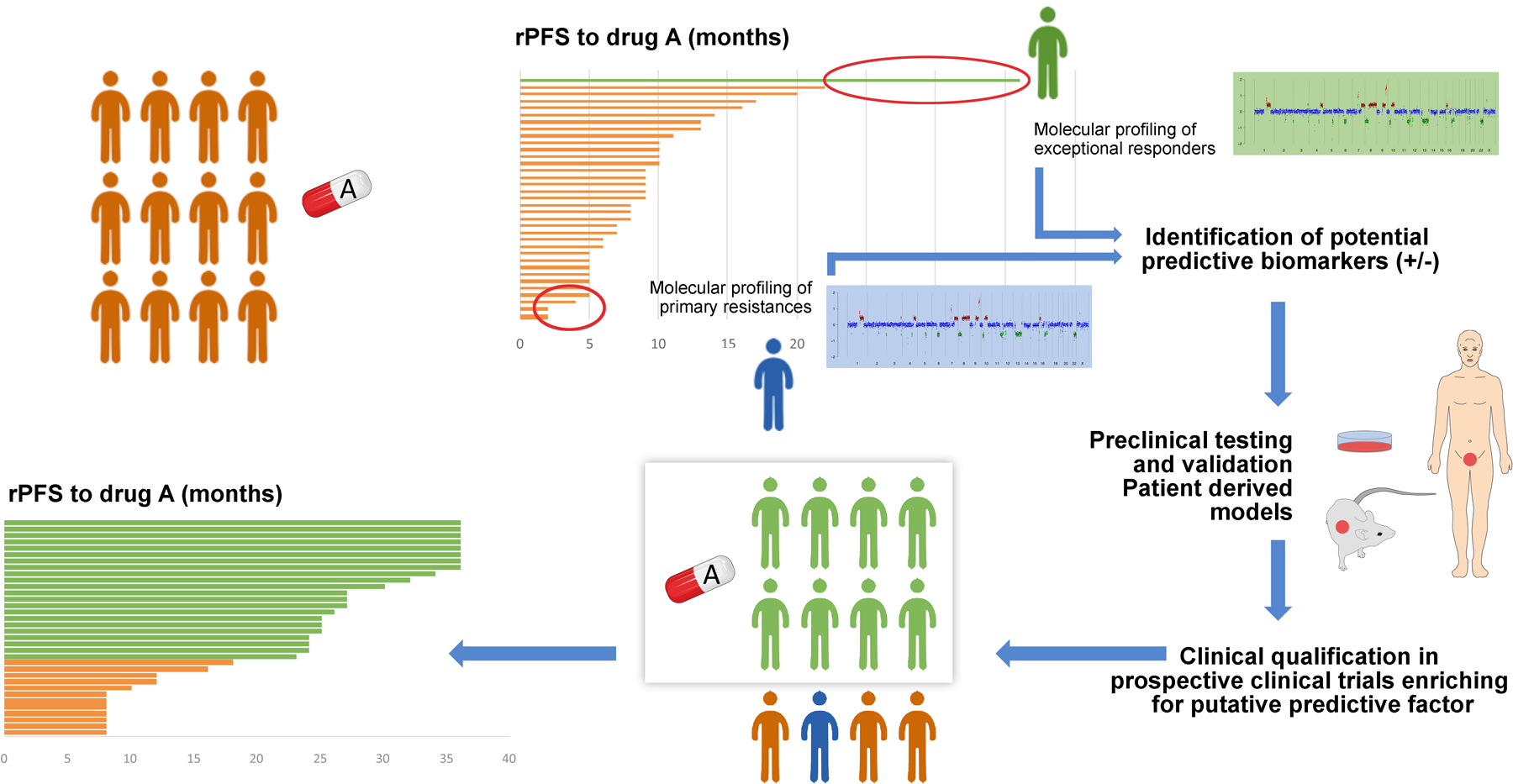
Despite advances in prostate cancer screening and treatment, available therapy options, particularly in later stages of the disease, remain limited and the treatment-resistant setting represents a serious unmet medical need. Moreover, disease heterogeneity and disparities in patient access to medical advances result in significant variability in outcomes across patients. Disease classification based on genomic sequencing is a promising approach to identify patients whose tumors exhibit actionable targets and make more informed treatment decisions. Here we discuss how we can accelerate precision oncology to inform broader genomically-driven clinical decisions for men with advanced prostate cancer, drug development and ultimately contribute to new treatment paradigms.
Conflict of interest statement
Competing Interests Statement. J.M. reports advisory board participation for Amgen, AstraZeneca, Roche, Janssen, MSD and Clovis Oncology; research funding from AstraZeneca and Pfizer Oncology; W.A. reports consulting /advisory for Clovis, Janssen, More Health, ORIC, Daiichi Sankyo; research funding from AstraZeneca, Zenith Epigenetics, Clovis, GlaxoSmithKline, ORIC, Epizyme; travel from GlaxoSmithKline, Clovis, ORIC; and honoraria from CARET. R.R.M. received research funding from Bayer, Pfizer, Tempus; serves on Advisory Board for Bayer, Bristol Myers Squib, Exelixis, Janssen, Novartis, Pfizer, Sanofi, Tempus; is a consultant for Dendreon, Vividion. R.A. reports advisory board participation and research funding from Merck, AstraZeneca, and Janssen; B.M. reports research funding from AstraZeneca, Janssen, Clovis, Astellas, Beigene; M.R. reports consulting: Amgen, Ambryx, Constellation; educational writing and consulting: Plexus; speaking: Bayer, Janssen; funding and clinical research support: Novartis, Astellas, Medivation, Merck; D.B.S. has consulted for/received honoraria from Pfizer, Loxo Oncology, Lilly Oncology, BioBridge, Vivideon Therapeutics, and Illumina; E.V. reports advisory/consulting: Tango Therapeutics, Genome Medical, Invitae, Enara Bio, Janssen, Manifold Bio, Monte Rosa; research support: Novartis, BMS; Equity: Tango Therapeutics, Genome Medical, Syapse, Enara Bio, Manifold Bio, Microsoft, Monte Rosa; travel reimbursement: Roche/Genentech; institutional patents on chromatin mutations and immunotherapy response, and methods for clinical interpretation; D.V. reports honoraria from Clovis Oncology. H.B. reports advisory/consulting from Janssen, Amgen, Astra Zeneca, Pfizer, Astellas, Sanofi Genzyme and research funding from Janssen, Abbvie Stemcentryx, Eli Lilly, Millenium, Astellas. J.V. is employed by the Prostate Cancer Clinical Trials Consortium. H.R.S., J.W.S., and A.K.M. are employed by the Prostate Cancer Foundation.
Figures
References
-
- Bray F et al. , Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68, 394–424 (2018). - PubMed
-
- Eggener SE et al. , Molecular Biomarkers in Localized Prostate Cancer: ASCO Guideline. J Clin Oncol 38, 1474–1494 (2020). - PubMed
-
- Sonni I et al. , Impact of. J Nucl Med, (2020).
-
- Klotz L et al. , Active Surveillance Magnetic Resonance Imaging Study (ASIST): Results of a Randomized Multicenter Prospective Trial. Eur Urol 75, 300–309 (2019). - PubMed
